Love Me Love My Phages -
Bacteriophages - The New Antibiotics-Part 2

The prospect for bacteriophage therapy in Western medicine.(Report)
Carl R. Merril, Dean Scholl, Sankar L. Adhya. Nature Reviews Drug Discovery. June 2003 v2 i6 p489(9).Author's Abstract:
Bacteriophage (phage) have been used for clinical applications since their initial discovery at the beginning of the twentieth century. However, they have never been subjected to the scrutiny -- in terms of the determination of efficacy and pharmacokinetics of therapeutic agents -- that is required in countries that enforce certification for marketed pharmaceuticals. There are a number of historical reasons for this deficiency, including the overshadowing discovery of the antibiotics. Nevertheless, present efforts to develop phage into reliable antibacterial agents have been substantially enhanced by knowledge gained concerning the genetics and physiology of phage in molecular detail during the past 50 years. Such efforts will be of importance given the emergence of antibiotic-resistant bacteria.
Full Text: COPYRIGHT 2003 Nature Publishing Group
Author(s): Carl R. Merril [1]; Dean Scholl [1]; Sankar L. Adhya [2]
The first widely used antibiotic, penicillin, was discovered 75 years ago. Since then, the production of antibiotics has grown into an industry with a market value estimated to exceed US $25 billion per year. Although antibiotics have saved countless lives, their widespread use has contributed to an increase in the incidence of antibiotic-resistant bacterial strains. For example, at the beginning of the antibiotic era Streptococcus pneumoniae was highly sensitive to penicillin, yet now, in some regions of the world, 25% of S. pneumoniae strains are resistant [1]. In addition, 70% of hospital-acquired bacterial infections in the United States are now resistant to one or more of the main antibiotics [2] and greater than 50% of clinical Staphylococcus aureus isolates in Japan are now multidrug resistant [3]. However, antibiotics are only one example of antibacterial entities that have arisen through the evolutionary competition between other species and bacteria. Another entity, the bacterial viruses (bacteriophage or PHAGE), might provide an alternative to fill the space created in the physician’s toolkit left by the dearth of new medicines to combat infections with antibiotic-resistant bacteria (Fig. 1).
The ability of phage to replicate exponentially and kill pathogenic strains of bacteria indicates that they should play a vital role in our armamentarium for the treatment of infectious diseases. In fact, such an application for phage was apparent to Felix d’Herelle after they were discovered by Twort in 1915 (Refs 4,5). d’Herelle was encouraged by his early experiments, in which he used phage to treat avian typhosis in chickens, shigella dysentery in rabbits and humans with bacillary dysentery. Following the reported successes of these experiments, d’Herelle travelled around the world stimulating basic and clinical phage research. Inspired by d’Herelle, the British medical officer Lieutenant Colonel Morison used phage for the prophylactic treatment of cholera epidemics in the Naogaon region of India from 1930 to 1935. In 1932, Morison reported few cholera deaths in the phage-treated Naogaon region, in contrast to the 474 deaths recorded in the Habiganj region which refused treatment [6, 7].
d’Herelle was also important in the establishment of a phage institute in Tbilisi, Soviet Georgia. This institute produced large quantities of phage for antibacterial therapy during and immediately following the Second World War and the institute is still actively pursuing phage therapy applications. Applications of phage as pursued in the Soviet Union (as well as Poland) have been extensively reviewed [8, 9]. The authors of these reviews noted that the details of phage dosages are presented primarily as qualitative data and that clinical criteria were generally reported in a ’sketchy’ manner. For these reasons, most of the studies from Eastern Europe will not meet the present standards for pharmaceutical approval in countries that require certification based on the results of efficacy and pharmacokinetic studies in animals and humans.
There was also an interest, in the 1920s and 1930s, in phage therapy in the United States. The large pharmaceutical company Eli Lilly & Co. sold ’Staphylo jel’, and other phage ’jel’ labelled products, for the treatment of Streptococcus spp. and colon bacilli infections. E. R. Squibb & Sons and the Swan-Myers division of Abbott Laboratories marketed a bacteriophage filtrate preparation for Staphylococcus spp., and combined bacteriophage filtrate preparations for Staphylococcus spp. and colon bacilli, respectively [10]. Despite this initial enthusiasm for phage products, clinical failures, theoretical concerns and the overshadowing development of antibiotics resulted in the abandonment of phage therapy in the United States and much of Western Europe [10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20](TIMELINE).
Re-examination of potential efficacy
Despite the chequered history of phage therapy, concerns over the increased incidence of antibiotic resistance has led investigators to examine the possibility of developing phage therapy into a reliable clinical tool. In one recently published animal study, a vancomycin-resistant Enterococcus faecium strain was used to induce a fatal bacteraemia (within 48 hours) in mice. Treatment with a single intraperitoneal injection of phage 45 minutes after the bacterial challenge was sufficient to rescue 100% of the animals, and even when treatment was delayed until the animals were moribund, phage administration was able to rescue 50% of the mice [21]. Similar results have been obtained using phage to treat animals infected with methicillin-resistant S. aureus [22]. In addition, phage have been used to treat Acinetobacter baumanii or Pseudomonas aeruginosa and animals with local and systemic disease caused by Vibrio vulnificus [23, 24].
Phages are also capable of treating antibiotic-resistant intracellular pathogens. Broxmeyer et al . [25] have demonstrated that it is possible to use Mycobacterium smegmatis , an avirulent mycobacterium, as a vector to deliver the LYTIC PHAGE TM4 to treat intracellular mycobacterium infections (with either Mycobacterium avium or Mycobacterium tuberculosis ) in macrophages. Phages have also been effective in the treatment of non-systemic infections, such as gastrointestinal infections caused by enteropathogenic strains of Escherichia coli in calves, pigs and lambs and ileocecitis caused by Clostridium difficile in hamsters [26, 27, 28, 29]. Phages have also been shown to be effective in preventing the destruction of skin grafts by P. aeruginosa [30]. Terrestrial animals are not the only candidates for phage therapy, as recent studies have shown that phage can be used to treat bacterial diseases of fish in aquiculture [31], bacterial blight of geranium [32] and bacterial spot on tomatoes [33].
Phage pharmacokinetics
Although phage therapy has a long history, pharmacokinetic data are still rudimentary. Most clinical applications of phage therapy have relied on the oral administration of phage preparations. This choice offers the possibility of reducing side effects from contaminants, including ENDOTOXINS and EXOTOXINS, but it might not provide the most effective therapeutic regimen(s) [34]. Some early practitioners of phage therapy recognized the need for pharmacokinetic information. The first effort to obtain such data in 1921 led to the observation that phage injected into the circulatory system of rabbits could still be found in the spleen long after the elimination of phage from other organs or the blood [35]. This finding was corroborated by both qualitative and quantitative experiments, in which a decrease in phage titre in the blood of mice injected with a Staphylococcus phage (a decrease of four orders of magnitude of phage titres was observed 5 minutes after intravenous injection, and by seven logs two hours later) was attributed to elimination by the reticulo-endothelial system (RES) [17, 36].
The relative roles of the liver and spleen in this process were determined by using 51 Cr-labelled phage. In these experiments the liver phagocytosed more than 99% of the phage in the circulatory system and inactivated the phage at a higher rate than the spleen [37]. Antibodies associated with the ADAPTIVE IMMUNE SYSTEM were not involved in this process, as demonstrated by experiments using germ-free mice that had no detectable antibodies to the phage strain used. Systemically administered phages were rapidly eliminated from the circulation of the germ-free mice. Furthermore, these quantitative experiments demonstrated that the oral administration of phage was not an effective method for delivery to systemic sites [34] (Fig. 2). Recognition that the RES can remove a significant proportion of administered phage led to the development of a serial passage selection method to isolate phage mutants with a greater capacity to remain in the circulatory system of the mouse. These ’long-circulating’ phage mutants also proved to be more effective therapeutically [38].
In studying the pharmacokinetics of phage it should be noted that phage DNA, like any other foreign DNA, can get into mammalian cells and, on rare occasions, into chromosomes [39, 40, 41]. There have also been reports of phage-induced enzyme activity in mammalian cells, albeit at low levels, following exposure to phage or phage DNA [42, 43]. Although there are efforts underway to enhance the capability of phage to serve as vectors for targeted gene delivery in mammalian cells [44], there is evidence that in the natural setting such effects are normally minimal: phages are, for example, associated with bacteria in our colon, nose, throat and skin throughout our life span.
For nearly all pharmacological agents, information on drug distribution and clearance would be sufficient for pharmacokinetic studies. However, unlike most pharmaceuticals, phage can replicate exponentially. The exploitation of phage as antibacterial therapeutics requires knowledge of three dynamic components: the infected human, the infecting bacteria and the phage, and their complex interactions. Of these three dynamic components, two of them -- the bacteria and the phage -- are capable of exponential growth during the course of an infection and its treatment. Given this situation, it is crucial to ensure that the phage titres employed are sufficient for a successful therapeutic outcome (Fig. 3). To explore such parameters, Smith and Huggins used two experimental models, one in which mice were infected intracerebrally with E. coli K1 and another in which they were infected intramuscularly. Phage was administered intramuscularly in both of these studies. The phage levels were found to be highest in the infected tissues and they fell as the bacterial levels in the infected tissue decreased.
These results corroborated the earlier finding of Dubos et al . [18] that mice infected intracerebrally with Shigella dysenteriae were rescued by administering phage into the peritoneal cavity [45]. In these experiments, the survival of untreated animals was 3.6%, whereas the survival of phage-treated animals was 72%. In addition, phage levels were observed to increase at the site of the infection -- the brain -- whereas the blood levels of phage seemed to be a "reflection of the events occurring in the brain". In uninfected control animals injected with phage, phage levels in the blood were compatible with the dilution of the phage in the total blood volume of the mouse. These researchers also showed that heat-inactivated phage provided no protective effects unless given days before the bacterial infection, and suggested that the protective effect of such heat-inactivated phage might result from the activation of antibacterial immunity by bacterial products present in the phage LYSATE.
Levin and Bull [46], and Payne and Jansen [47], have developed formal mathematical models on the basis of data from the Smith and Huggins [26] study. The Payne and Jansen [47] model included terms for the loss of phage resulting from interaction with mammalian systems, such as the RES. Their analysis with this model corroborated the suggestion by Alinsky et al . [8] that antibiotic and phage therapies might not be synergistic. Although such models are important for pharmacological planning, present efforts are based on limited datasets. Recently developed methods of visualizing bacterial infections in live animals using bioluminescent strains of bacteria might help in such pharmacokinetic studies [48]. This method uses a high sensitivity charge-coupled device camera to monitor bacteria in live mice. The bacteria are made bioluminescent by incorporating a luciferase transposon cassette into their genome. As it is feasible to incorporate luciferase transposon cassettes into phage genomes, it should also be possible to follow phage interactions with bacterial infections in vivo .
Phage immunogenicity
Phage immunogenicity is important for two reasons: first, because of potential adverse reactions, such as anaphylactic shock, and second, because of its effects on the pharmacokinetics of phage therapy. When phage are first used, some behave as NEO-ANTIGENS, as there are no pre-existing antibodies for these phage. This feature, along with the lack of apparent side effects, has permitted the use of phage [phi]X174 as a probe of human and animal immune sytems [49, 50, 51]. Despite the apparent lack of antibodies to phage that present as neo-antigens they still interact with the innate immune system, as demonstrated by the rapid loss of phage injected into the circulatory system of germ-free mice [34] and the capacity of the liver to phagocytose more than 99% of administered phage within 30 minutes of inoculation [37]. It is important to note that not all phage present as neo-antigens, as Kucharewica-Krukowska and Slopek noted in a study in which 11% of their healthy controls and 23% of their patients had antibodies against a Staphylococcus phage strain before administration of phage therapy [45].
If a particular phage strain were used repeatedly as an therapeutic antibacterial agent, in addition to the interactions with the innate immune system, the adaptive immune system would be stimulated and result in the production of antibodies. Such activation of the adaptive immune system relies on somatic mutations and clonal expansion of T and B cells, which can take at least three to five days. In normal individuals injected with the highly immunogenic phage [phi]X174, the phage is normally cleared within three days and a primary immunoglobulin M (IgM) response can be observed that peaks two weeks after the initial injection or immunization. If another injection is made six weeks later, the IgM and IgG antibody titres increase and peak within one week of the second injection; subsequent phage injections result in further increases in the IgG titres [50]. Patients with severe combined immune deficiency (SCID), which is characterized by the absence of both B and T cell functions, display a prolonged period for the clearance of phage, with phage present up to four to six weeks after the initial injection. In addition, SCID patients do not develop detectable antibody responses to phage, even after repeated injections. Ochs and his colleagues have also found that although [phi]X174 phage is a potent antigen, it causes no recognized toxic effects in man [49, 52].
Similar findings were reported for the phage ENB6 used to treat mice infected with vancomycin-resistant Enterococcus [21]. To determine the immunogenicity of this phage, mice were given monthly injections. After the third in a series of five monthly injections, the titres of IgG and IgM increased 3,800-fold and fivefold, respectively, above background. The IgG levels did not change substantially after the third phage injection. No anaphylactic reactions, changes in core body temperature or other adverse events were observed in the mice over the course of these multiple injections of phage [21]. It might be possible to develop phage that are less antigenic by using phage-displaying peptide libraries or affinity matrixes made up of antibodies from human serum. This type of approach has been initiated to decrease the immunogenicity of therapeutically important enzymes [53].
Bacterial host specificity of phage
The bacterial host range of phage is generally narrower than that found in the antibiotics that have been selected for clinical applications. Most phage are specific for one species of bacteria and many are only able to lyse specific strains within a species. This limited host range can be advantageous, in principle, as phage therapy should result in less harm to the normal body flora and ecology than commonly used antibiotics, which often disrupt the normal gastrointestinal flora and result in opportunistic secondary infections by organisms such as C. difficile [54]. The potential clinical disadvantages associated with the narrow host range of most phage strains can be addressed through the development of a large collection of well-characterized phage for a broad range of pathogens, and methods to rapidly determine which of the phage strains in the collection will be effective for any given infection.
Ideally, broad-host-range phage should be selected for therapeutic applications. However, if such phage strains cannot be found, present molecular techniques can be used to enhance the host range of some phage strains. For example, it has been found that coliphage K1-5 is a ’dual’ specificity phage that encodes two different tail proteins; this allows it to attack and replicate in both K1 and K5 strains of E. coli [55]. One tail protein found on phage K1-5 is a lyase protein, similar to that of phage K5 (specific for the K5 polysaccharide capsule), and a second tail protein found on this phage is an ENDOSIALIDASE similar to a tail protein found in phage K1E (specific for the K1 polysaccharide capsule). In addition, the genomic region encoding these proteins is almost identical to the genomic construct found in the salmonella phage SP6, which codes for a protein that binds to the salmonella O-antigen [56]. The observation of a similar tail genome motif in both the salmonella phage SP6 and the coliphages K1E, K5 and K1-5 indicates that this genomic construct might serve in the development of a modular phage platform that could operate over a wide bacterial host range.
Other mechanisms have been found that permit expansion of the bacterial host range of phage. These include the site-specific recombination systems that permit phage to switch between alternative tail fibre proteins [57] and the use of a reverse transcriptase, possessed by a Bordetella phage, to generate variation in its tail fibre proteins [58]. Such expanded host-range ’platform’ phage would provide for versatility and save time and effort compared with that required for the development of completely new phages for each bacterial strain.
Other factors can affect host specificity. For example, bacterial restriction/modification systems might limit the host range of some phage. This problem could be addressed, in principle, by engineering phages with genomes that do not contain restriction sites recognized by the non-permissive host. Alternatively, phages could be produced in bacterial strains that provide DNA modification(s) that allow the phage to escape restriction in the targeted strain of bacteria. Another approach would be to incorporate genes into the phage genome that facilitate inhibition of bacterial restriction/modification enzymes, as exemplified by the mechanism used by the phage T7 which encodes an antirestriction enzyme [59]. A construct containing such an antirestriction gene might be adapted for use in other phage strains, or it might be possible to modify T7 phage to expand its bacterial host range for E. coli infections.
Phage growth: in vitro versus in vivo
In addition to the factors addressed above, bacteria grown with standard laboratory protocols can behave differently in the milieu of an infection. Bacteria possess feedback mechanisms that can alter their gene expression in response to changing environmental conditions. Such variations in gene expression can affect phage susceptibility. For example, Karakawa noted that S. aureus rarely expresses the capsular polysaccharides found in clinical isolates when the bacteria are grown in the laboratory [60]. Given the possibility for such changes in the bacterial capsule, phage discovered using bacteria grown in vitro might not be able to multiply in an infected animal. Recently, it has been reported that phage that infected certain strains of E. coli that did not express the cell surface protein Ag43 in standard laboratory growth media can be inhibited by concentrations of bile salts similar to that found in the gastrointestinal tract [61]. In this case, the bile salts might affect the expression of the Ag43 protein, which has been shown to be a phase -variable protein whose expression is associated with E. coli BIOFILM formation [62].
In addition, different in vitro and in vivo bacterial densities can be important [47]. Variations in phage physiology also are important, as some phage infections cause the host bacteria to release lysins that result in the destruction of bacteria not directly infected by the phage ([Box 1] and Fig. 4). In the early phage literature, there are reports of body fluids (for example, serum, pus, ascites fluids, cerebrospinal fluid, urine and bile) that inhibit the infectivity of phage that were active in vitro against typhoid, colon bacilli and staphylococci [63, 64]. Some of these effects might have resulted from alterations of bacterial physiology.
Detrimental phage genes
Some phage strains, the lytic phage, kill bacteria, whereas others -- LYSOGENIC or temperate phage -- have a dual life style: they can either kill and lyse their bacterial host or become quiescent by integrating their genome into their bacterial host chromosome. Some lysogenic phage encode toxins or factors that enhance bacterial pathogenesis (Table 1). Phage can also contribute, through transduction, to the transmission of antibiotic-resistance genes [65]. It is essential that phage considered for therapeutic applications be screened for toxin genes, either biochemically or by sequencing their DNA. The presence of toxin, antibiotic resistance genes, and genes that increase bacterial pathenogenicity, can be checked by searching phage genomes against GenBank online using the Basic Local Alignment Search Tool (BLAST) [66] and other similar programs. Success cannot be assumed as we are still in the discovery stage of such detrimental genes. The usefulness of bioinformatic analysis will increase as knowledge of these potential deleterious genes accumulates.Selection of therapeutic phage strains
The narrow host range of most phage strains dictates the need for the rapid determination of bacterial susceptibility. The determination of suitable therapeutic phage strain(s) using traditional procedures can take days to accomplish, limiting the use of phage therapy to slowly progressing infections. However, recent methods have been developed that permit the identification of both the infectious agent and a suitable phage strain within a day or less.One such approach uses of phage that contain reporter genes, such as luciferase [67, 68]. For example, a collection of phage strains, each encoding luciferase protein, could be individually placed in a multi-well plate. When a clinical sample, such as urine or sputum, is added to the wells, light will be emitted and detected in those wells that contain a phage strain that successfully infects the bacteria in the clinical specimen. Such light emission would serve to identify both bacterial strains and the phage strains that could be used against them. This test could be performed in hours, instead of the days that traditional culture methods require. This approach has been used to detect Listeria contamination in foods [67] and in an inexpensive and rapid diagnostic test for tuberculosis [68]. Alternatively, similar results can be achieved by using phage that do not have such marker genes, by placing luciferin and luciferase in the phage/bacterial incubation mixture in each of the wells of the multi-well plate. The lysis of bacterial strains by a phage strain in any of the wells will result in the discharge of adenylate kinase into the well, which will convert the ADP in the reaction mix to ATP. As the luciferin/luciferase system can utilize the ATP for light emission, lysis will serve to identify phage susceptibility without the need to genetically engineer the phage with a luciferase reporter gene [69].
Another method for the rapid identification of bacterial strains could be provided by mass spectrometry (MS). Mass fragment ’fingerprints’ of lipid, protein and nucleic acid bacterial components are used at present for rapid strain identification [70, 71]. It might also be possible to use this approach to determine whether bacteria are susceptible to a particular phage strain. However, such information is not available at present and it might be impractical to gain sufficient knowledge of bacterial mass fingerprints to determine which phage strains to use therapeutically for a bacterial host responsible for an infectious disease. Alternatively, phage gene products might provide for the development of markers for both bacterial identification and as an indicator of phage susceptibility. In this approach, one could use MS by placing a clinical sample in growth media to amplify the infecting bacteria followed by exposure to selected ’therapeutic’ phage strains. If the bacteria were susceptible to the phage, MS would detect signature fragments of phage proteins that are expressed only when infection of the bacteria occurs by a specific phage. Such ’signature’ fragments, that are not part of the phage virion, would be generated from phage: RNA polymerase, regulatory protein or lytic enzymes.
DNA microarray technologies also offer possibilities for determining bacterial strains in disease states and possibly the phage strains that might be used therapeutically. DNA microarrays, in conjunction with polymerase chain reaction, are now being developed for the rapid diagnosis of bacterial strains and antibiotic susceptibility [72]. In principle, it might be possible to develop such methods for the determination of bacterial strains and their phage susceptibility.
Development and preparation of phage
In addition to biological factors, phage preparative methods are crucial for the development of reliable phage therapeutics. Early therapeutic applications used impure phage preparations with deleterious clinical effects ([Box 2]). Contamination of phage preparations can result in increased morbidity or, in some cases, mortality. For example, in a recently published study, intraperitoneal inoculation of mice with filter-sterilized phage lysates produced reactions associated with endotoxin levels that ranged from mild (ruffled fur) to death [38]. Adequate purification, for example, by physical and/or biochemical methods, must be adopted for the production of toxin-free, clinical-grade phage preparations with long-term storage stability [38, 73]. Phage prepared in this manner have been administered to animals without any noticeable ill effects and Ochs et al . have used such purified phage in their human protocols [49].
In developing phage purification procedures, testing for adverse effects should not be limited to observation with healthy animals. Individuals that are under stress can have a lowered tolerance to endo- and exotoxins. In a recent mouse bacteraemia study, a lower survival rate was observed in a ’control experiment’ in which a phage strain, known to be inactive against the bacterial strain being used at the LD50 level, was administered to the infected mice. Although the highest doses of this phage preparation produced no apparent adverse effects in healthy uninfected animals, an increased mortality was observed in the bacteraemia-stressed mice. This increased mortality was phage-dose dependent, indicating that stressed animals are more sensitive to the phage itself, or to the trace amounts of endo- and exotoxins present in the phage preparations, than normal animals [21]. This example provides additional evidence for the need for highly purified phage preparations for therapeutic applications.
It should also be noted that bacteriostatic or bacteriocidal agents, used to ensure that no active bacteria are present in phage preparations, can also be detrimental. The association between ’weak’ phage preparations and the presence of organomercury compounds was made in a 1932 study of commercial phage preparations from a large US pharmaceutical company [10].
Future prospects
Although results from animal experiments are encouraging, continuing research will be needed to develop phage therapy for the treatment of human infectious diseases. These efforts should include studies of phage genomics, pharmacokinetics and efficacy in animal models of infectious diseases. In addition, phage chosen for therapeutic applications will need to be screened to reduce the chance that they carry genes encoding toxins, or factors that enhance bacterial pathogenicity. Phage growth, purification and storage protocols are needed to assure therapeutic efficacy and to reduce the possibility of contamination of pharmaceutical preparations by toxins and bacterial debris. Furthermore, the narrow host range of most phage strains requires the development of rapid methods for the determination of appropriate phage strains for use in specific infections.
Development of therapeutic phage could provide some relief from the growing threat from the emerging antibiotic-resistant bacterial strains and, as Lederberg suggested, treatments for epidemics such as cholera in refugee camps [74]. In addition, the narrow host range of phage could be better suited than presently employed antibiotics to a number of clinical applications. For example, the lack of genetic variability in antibiotic-resistant bacteria suggests that the resulting pathogenic bacteria might offer ideal targets for phage therapy. Only 10 strains of Pneumococcus are associated with 75% of the cases of antibiotic-resistant childhood pneumonia, and one-half of these cases are caused by the single strain ’Spain 23-E’. Herminia de Lencastre obtained similar results in a study of methicillin-resistant S. aureus , in which only five strains of methicillin-resistant S. aureus were found in 70% of 3,000 clinical isolates from 14 countries [75]. The narrow host range of phage should also reduce the disturbance of the complex bacterial ecological systems associated with the human gastrointestinal system. Applications of phage to treat infections could eliminate the IATROGENIC effects of antibiotics, such as the antibiotic-related diarrhoea diseases that range from ’nuisance’ diarrhoea to colitis associated with C. difficile infections [55].
Phage, with their narrow host range, could also prove useful in treating bacterial infections in agricultural applications without disturbing larger ecological systems, as is often the problem with antibiotics [74]. This suggestion is strengthened by the recent observations that many antibiotic-resistant bacterial strains are arising through clonal selection. In recognition of this growing problem, the FDA recently announced that it is re-evaluating livestock antibiotics, and it is now requiring manufacturers of proposed livestock antibiotics to determine whether these proposed antibiotics will be associated with the emergence of pathogenic organisms with resistance to drugs presently in use for the treatment of human diseases [76].
In regard to concerns over regulatory agency approval, it should be noted that phage have been used successfully as a means to probe immune-deficiency diseases in human studies for the past three decades [49, 50]. In addition, some vaccines were found, in the 1970s, to be contaminated with phage. An executive order was issued to permit the continued use of these contaminated vaccines [77, 78]. We should also recognize that we are normally in contact with phage throughout our lifetime, with the complex interactions of bacteria and phage in our colon, upper respiratory system and on our skin. In fact, many present phage collections were derived from human waste.
It is clear from recent experiments that phage therapy has the potential to rescue animals infected with antibiotic-resistant bacterial stains [22, 21]. We now also have much of the knowledge needed to develop phage into reliable therapeutic preparations. Whether we embark on efforts needed to develop therapeutic phage for human infections depends in part on our need to obtain relief from the growing threat of emerging antibiotic-resistant bacterial strains and our will to accomplish this task.
Definition List:
ADAPTIVE IMMUNE SYSTEM: The arm of the immune system that mounts an antigen-specific immune response as the result of the clonal selection of antigen-specific lymphocytes. Such lymphocytes produce antibodies that react with the antigen. The adaptive immune responses differ from the innate and non-adaptive immune system, which does not depend on clonal selection of antigen-specific lymphocytes.
BIOFILM: A structure made up of a community of bacteria composed of microcolonies and water channels that survives at a liquid interface. Such biofilms play a role in the pathogenic effects of bacterial infections associated with gingivitis, colitis, vaginitis, urethritis, conjunctivitis and otitis.
ENDOTOXINS: Components of bacterial cells that are usually associated with the lipopolysaccharide components of the outer layer of Gram-negative bacterial cell walls that are toxic (to mammals). Endotoxins are released in large quantities upon lysis of Gram-negative bacterial cells.
ENDOSIALIDASES: Enzymes that cleave at the sialic acid residue sites of the complex oligosaccharides associated with the protective capsule of many bacterial strains.
EXOTOXINS: A broad class of factors released by pathogenic bacteria that can harm infected mammals. Examples of such exotoxins are botulism toxin (Clostridium botulinum ), streptolysins (Streptococcus pyogenes ) and diphtheria toxin (Corynebacterium diptheriae ).
IATROGENIC: An effect that is induced in a patient by a physician’s activity or therapy; such effects often occur as complications of treatments for infectious diseases.
LD50 : The amount of a substance that causes the death of 50% of test subjects.
LYSATE: The colloidal bacterial growth media remaining after phage replicate and kill the host cells. Lysates contain phage progeny, bacterial cell wall debris and, often, internal cellular components (for example, proteins, nucleic acids, small molecules and so on).
LYSOGENIC PHAGE: Phage that are capable of integrating their genome (that is, lysogenize) into the host chromosome. Such phages often mediate horizontal gene transfer (transduction) between bacterial strains. Most lysogenic phage can also go through a lytic cycle to produce more phage, often after induction (from some environmental factor).
LYTIC PHAGE: Phage that infect bacterial cells to replicate and then lyse the bacterial host.
NEO-ANTIGEN: An antigen for which animals or humans being studied have no pre-existing antibodies. The phage [phi]X174, which is highly immunogenic, has served as such a neo-antigen in studies of human antibody responses, as most humans have no pre-existing antibodies to this phage.
PHAGE: Bacterial viruses. The term phage is used as both singular and plural when referring to phage(s) that is/are member(s) of a single phage strain. However, when referring to phage in more than one strain the plural is phages.
PHAGE PLAQUE: The lesion formed when a phage particle is applied to a film of a susceptible bacterial strain that is growing on an agar surface. The lesion results from the infection of a bacterial cell by a phage particle, followed by the production of phage progeny and their release by lysis, followed by the infection and lysis of additional bacterial cells in the vicinity of the initial infection.
Web Link(s):
DATABASES
Online Mendelian Inheritance in Man
Severe combined immunodeficiency: http://www.ncbi.nlm.nih.gov/htbin-post/Omim/dispmim?102700
FURTHER INFORMATION
Encyclopedia of Life Sciences
Bacteriophages: http://www.els.net/els/FDA/default.asp?id=25CA4A8E-4CC9-4DCE-9E33-D5DD1D5A2AE2
bacteriophages in industry: http://www.els.net/els/FDA/default.asp?id=5CF03976-9CBE-4DCB-9A53-D4CBFA9BD344
phage display technologies: http://www.els.net/els/FDA/default.asp?id=CED7B675-3979-43EF-BB87-8EE22D7BE08C
Genomes of the T4-like Phages: http://phage.bioc.tulane.edu/
Phage Ecology and Evolutionary Biology: http://www.mansfield.ohio-state.edu/~sabedon/
Phage Page: http://www.mbio.ncsu.edu/esm/phage/phage.html
Phage Therapy: http://www.evergreen.edu/phage/phagetherapy.html
Therapeutic uses of phage: http://surfer.iitd.pan.wroc.pl/phages/phages.html
Box 1 | Therapeutic use of phage products
Phage gene products might also serve as therapeutic agents. Although such applications lack the exponential growth capacity of phage, they could still be highly effective. For example, the small-genome phages [phi]X174 and Q[beta] encode polypeptides that could be developed into a new class of antibiotics, as they interfere with bacterial cell wall biosynthesis [79]. Such inhibition results in bacterial lysis. Similarly, phage-encoded endolysins that disrupt the peptidoglycan matrix of the bacterial cell wall, and phage-encoded holins that permeabilize bacterial membranes, can also serve as effective antibacterial agents. A phage lysin, specific for streptococci groups A, C and E, has been used to treat experimental upper respiratory infections in mice [80].
Such lysins should be less disruptive than most antibiotic treatments as they have little, if any, effect on other commensal organisms in the oral and upper respiratory tract. In another example, the [gamma] phage of Bacillus anthracis encodes a lysin that proved to be effective in rescuing mice infected with Bacillus cereus , a bacterial strain closely related to B. anthracis [69]. No resistant B. cereus strains were detected following such treatment. In addition, phage lysin genes have been incorporated into bacterial genomes for prophylactic applications. Gaeng et al . [81] developed such a bacterial strain to secrete the functional phage lysin enzymes Ply511 and Ply118 to reduce Listeria monocytogenes contamination in dairy cheese production starter cultures [81].
These phage lysins can also be used diagnostically. For example, when PlyG lysin destroys B. anthracis , ATP is released, which, in conjunction with the luciferin/luciferase system, results in the emission of light that can also be used to rapidly detect bacilli and their germinating spores. This system was able to detect as few as 100 spores [69].
Box 2 | Therapeutic failure that might have resulted from impure phage
Some of the early clinical therapeutic failures might have been due to inadequate purification of the phage preparations. In one such example, reported in 1932, a phage strain was found that seemed to be promising as a therapeutic agent as it could lyse cultures of plague (Yersinia pestis ) grown in broth media in less than 2 hours. However, when this phage strain, purified solely by filtration, was injected into rabbits experimentally infected with Y. pestis , the mortality increased to levels above those found in infected rabbits that were not treated with phage. Furthermore, when this phage preparation was used to treat 33 human patients, they all died. The mortality from plague is normally 60-90% [82].
Caption(s):
Illustration 1: Timeline | Highlights in the development of phage as a potential therapeutic agent for bacterial infections [see PDF for image]
Figure 1: Electron micrograph of phage. [see PDF for image]
This is an Escherichia coli phage. Phage can range from filamentous to spherical structures. However, many of them have a distinct head, containing their DNA, and a tail-like structure that can bind to bacterial receptors.
Figure 2: Systemic distribution of phage following intravenous and oral administration of phage. [see PDF for image]
These experiments demonstrate that oral administration is not an effective method for the delivery of phage to systemic sites as the blood and tissues levels were seven to eight orders of magnitude lower with oral administration than those achieved by systemic administration of phage. pfu, plaque-forming units.
Figure 3: The effect of therapeutic phage concentration on morbidity and mortality. [see PDF for image]
When phage are used to treat a systemic bacterial infection, the concentration of phage administered must be adequate to kill the infecting bacteria before they can kill the mammalian host. This point is illustrated in the data, from a study using phage to treat bacteraemic mice infected with 109 colony-forming units (cfu) of vancomycin-resistant Enterococcus faecium [21]. This concentration of bacteria normally results in death within 48 hours. Each bar represents a single mouse, and all but the two control mice (injected with buffer rather than bacteria, represented by the pink bars) were infected with 109 cfu of bacteria. The phage concentrations administered 45 minutes after the bacterial infection are depicted in the key. The mice in the last group (red bars) did not receive phage therapy. The state of health scale is a non-parametric scale in which: 5 = normal; 4 = decreased activity and ruffled fur; 3 = lethargy, ruffled fur and hunchback posture; 2 = hunchback posture and partially closed eyes with exudates; 1 = moribund; and 0 = death. pfu, plaque-forming units.
Figure 4: Phage plaques on a bacterial ’lawn’. [see PDF for image]
The PHAGE PLAQUES illustrated on this plate display a mixture of morphologies, which reflect the different phage strains applied to this bacterial plate. Some of the phage produce small clear plaques, whereas other phage strains that produce lysins have a clear centre zone surrounded by a spreading zone of killing.
Table: Phages that carry toxin genes and their gene products [83] [see PDF for image]
References
1. Thornsberry, C. et al . Regional trends in antimicrobial resistance among clinical isolates of Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis in the United States: results from the TRUST Surveillance Program, 1999-2000. Clin. Infect. Dis. 34, S4-S16 (2002).
2. National Center for Infectious Diseases. Campaign to prevent antimicrobial resistance in healthcare settings. Centers for Disease Control and Prevention [online] (cited 30 Sep 2002) <http://www.cdc.gov/drugresistance/healthcare/problem.htm> (2002).
3. Hashimoto, H. Drug resistance of methicillin-resistant Staphylococcus aureus (MRSA) in Japan until 1993. Jpn J. Antibiot. 47, 575-584 (1994).
4. Twort, F. W. An investigation on the nature of ultra-microscopic viruses. Lancet 2, 1241-1243 (1915).
This paper presents the original discovery of bacterial viruses.
5. d’Herelle, F. The Bacteriophage and its Behavior 490-541 (Williams & Wilkins, Baltimore, Maryland, 1926).
Although much of the material in this book is dated, it still contains observations of interest.
6. Summers, W. C. Felix d’Herelle and the origins of Molecular Biology 125-144 (Yale University Press, New Haven and London, 2001).
7. Summers, W. C. Bacteriophage therapy. Annu. Rev. Microbiol. 55, 437-451 (2001).
8. Alinsky, J., Iczkowski, K., Rapoport, A., & Troitsky, N. Bacteriophages show promise as antimicrobial agents. J. Infect. 16, 5-15 (1998).
This and the following article present an overall review of phage therapy efforts in Poland and the Soviet Union.
9. Sulakvelidze, A., Alavidze, Z. & Morris, J. G. Jr Bacteriophage therapy. Antimicrob. Agents Chemother. 45, 649-659 (2001).
10. Straub, M. E. & Applebaum, M. Studies on commercial bacteriophage products. JAMA 100, 110-113 (1933).
Insights into the problems associated with pharmaceutical phage preparations.
11. Larkum, N. W. Bacteriophage in clinical medicine. J. Lab. Clin. Med. 17, 675-680 (1932).
12. Van Helvoort, T. Bacteriological and physiological research styles in the early controversy on the nature of the bacteriophage phenomenon. Med. Hist. 36, 243-270 (1992).
13. Randall-Hazelbauer, L. & Schwartz, M. Isolation of the bacteriophage [lambda] receptor from Escherichia coli . J. Bacteriol. 116, 1436-1446 (1973).
14. Eaton, M. D. & Bayne-Jones, S. Bacteriophage therapy. JAMA 103, 1769-1776, 1847-1853 & 1934-1939 (1934).
15. Ho, K. Bacteriophage therapy for bacterial infections. Perspect. Biol. Med. 44, 1-16 (2001).
16. Barrow, P. A. & Soothill, J. S. Bacteriophage therapy and prophylaxis: rediscovery and renewed assessment of potential. Trends Microbiol. 5, 268-271 (1997)
17. Evans, A. C. Inactivation of antistreptococcus bacteriophage by animal fluids. Public Health Rep. 48, 411-426 (1933).
18. Dubos, R. J., Straus, J. H. & Pierce, C. The multiplication of bacteriophage in vivo and its protective effects against experimental infection with Shigella dysenteria . J. Exp. Med. 20, 161-168 (1943).
This paper presents crucial experiments designed to explore the mechanisms underlying the therapeutic effects observed when using phage to treat a systemic bacterial infection.
19. Asheshov, I. N., Wilson, J. & Topley, W. W. C. The effect of an anti-vi bacteriophage on typhoid infection in mice. Lancet 319-320 (1937).
20. Stent, G. S. Molecular Biology of Bacterial Viruses (W. H. Freeman, San Francisco, 1963).
Essential information for those interested in phage and their applications, and provides insights into theories concerning phage therapy failures.
21. Biswas, B. et al . Bacteriophage therapy rescues mice bacteremic from a clinical isolate of vancomycin-resistant Enterococcus faecium . Infect. Immun. 70, 204-210 (2002).
In addition to a demonstration of the effectiveness of phage therapy for treatment of animals infected with antibiotic resistant bacteria, the experiments in this study also show that the rescue of infected animals is directly dependent on phage function.
22. Matsuzaki, S. et al . Experimental protection of mice against lethal Staphylococcus aureus infection by novel bacteriophage MR11. J. Infect. Dis. 187, 613-624 (2003).
The animal experiments described in this paper provide evidence that phage could provide an alternate therapeutic approach for the treatment of a serious antibiotic-resistant bacterial infection.
23. Soothill, J. S. Treatment of experimental infections of mice with bacteriophages. J. Med. Microbiol. 37, 258-262 (1992).
24. Cerveny, K. E, Depaola, A., Duckworth, D. H & Gulig, P. A. Phage therapy of local and systemic disease caused by Vibrio vulnificus in iron-dextran-treated mice. Infect. Immun. 70, 6251-6262 (2002).
25. Broxmeyer, L. et al . Killing of Mycobacterium avium and Mycobacterium tuberculosis by a mycobacteriophage delivered by a nonvirulent mycobacterium: a model for phage therapy of intracellular bacterial pathogens. J. Infect. Dis. 186, 1155-1160 (2002).
Intracellular bacterial infections are often difficult to treat and this paper provides evidence that phage could provide a therapeutic approach to this problem.
26. Smith, H. W. & Huggins, M. B. Successful treatment of experimental E. coli infections in mice using phage: its general superiority over antibiotics. J. Gen. Microbiol. 128, 307-318 (1982).
This is a crucial study in which fewer resistant bacterial colonies were found following phage therapy than found following antibiotic therapies, and the phage-resistant bacterial colonies were reported to have alterations in their capsules associated with reduced pathogenic properties.
27. Smith, H. W., Huggins, M. B. & Shaw, K. M. The control of experimental E. coli diarrhea in calves by means of bacteriophages. J. Gen. Microbiol. 133, 1111-1126 (1987).
28. Smith, H. W., Huggins, M. B. & Shaw, K. M. Factors influencing the survival and multiplication of bacteriophages in calves and their environments. J. Gen. Microbiol. 133, 1127-1135 (1987).
29. Ramesh, V., Fralick, J. A. & Rolfe, R. D. Prevention of Clostridium difficile -induced ileocecitis with bacteriophage. Anaerobe 5, 69-78 (1999).
30. Soothill, J. S. Bacteriophage prevents destruction of skin grafts by Pseudomonas aeruginosa . Burns 20, 209-211 (1994).
31. Nakai, T. & Park, S. C. Bacteriophage therapy for infectious diseases in aquiculture. Res. Microbiol. 153, 13-18 (2002).
32. Flaherty, J. E., Harbaugh, B. K., Jones, J. B., Somodi, G. C. & Jackson, L. E. H-mutant bacteriophages as a potential biocontrol of bacterial blight of geraniums. Hortscience 36, 90-100 (2001).
33. Flaherty, J. E., Jones J. B., Harbaugh, B. K., Somodi, G. C. & Jackson, L. E. Control of bacterial spot on tomato in the greenhouse and field with H-mutant bacteriophages. Hortscience 35, 882-884 (2000).
34. Geier, M. R., Trigg, M. E. & Merril, C. R. The fate of bacteriophage [lambda] in non-immune germ-free mice. Nature 246, 221-223 (1973).
This paper highlights the distribution of functional phage administered by various routes in mice and it presents evidence that oral administration is an ineffective method for achieving a systemic distribution of phage.
35. Appelmans, R. Le bacteriophage dans l’organisme. Comp. Rend. Soc. de Biol. (Paris) 85, 722-724 (1921).
36. Nungester, W. J. & Watrous, R. M. Accumulation of bacteriophage in spleen and liver following its intravenous inoculation. Proc. Soc. Exper. Biol. Med. 31, 901-905 (1934).
37. Inchley, C. J. The activity of mouse kupffer cells following intravenous injection of T4 bacteriophage. Clin. Exp. Immunol. 5, 173-187 (1969).
The crucial role of the liver in removing phage from the circulation of mammals is clearly delineated in this study.
38. Merril, C. R. et al . Long-circulating bacteriophage as antibacterial agents. Proc. Natl Acad. Sci. USA 93, 3188-3192 (1996).
This paper describes the development of a selection technique, based on the recognition that the efficacy of phage therapy might be impaired by the mammalian innate immune system, for obtaining long-circulating phage with enhanced therapeutic properties.
39. Doerfler, W. et al . On the insertion of foreign DNA into mammalian genomes: mechanism and consequences. Gene 157, 241-245 (1995).
40. Schubbert, R., Hohlweg, U., Renz, D. & Doerfler, W. On the fate of orally ingested foreign DNA in mice: chromosomal association and placental transmission to the fetus. Mol. Gen. Genet. 259, 569-576 (1998).
41. Schubbert, R., Renz, D., Schmitz, B. & Doerfler, W. Foreign (M13) DNA ingested by mice reaches peripheral leukocytes, spleen, and liver via the intestinal wall mucosa and can be covalently linked to mouse DNA. Proc. Natl Acad. Sci. USA 94, 961-966 (1997).
42. Merril, C. R., Geier, M. R. & Petricciani, J. C. Bacterial virus gene expression in human cells. Nature 233, 398-400 (1971).
43. Horst, J., Kluge, F., Beyreuther, K. & Gerok, W. Gene transfer to human cells: transducing phage [lambda] plac gene expression in GM1-gangliosidosis fibroblasts. Proc. Natl Acad. Sci. USA 72, 3531-3535 (1975).
44. Larocca, D. et al . Evolving phage vectors for cell targeted gene delivery. Curr. Pharm. Biotechnol. 3, 45-57 (2002).
45. Kucharewica-Krukowska A. & Slopek S. Immunogenic effect of bacteriophage in patients subjected to phage therapy. Arch Immunol. Ther. Exp. (Warsz.) 35, 553-561 (1987).
46. Levin, B. R. & Bull, J. J. Phage therapy revisited: the population biology of a bacterial infection and its treatment with bacteriophage and antibiotics. Am. Nat. 147, 881-898 (1996).
47. Payne, R. J. H. & Jansen, V. A. A. Pharmacokinetic principles of bacteriophage therapy. Clin. Pharmacokinet. 42, 315-325 (2003).
48. Francis, K. P. et al . Visualizing Pneumococcal infections in the lungs of live mice using bioluminescent Streptococcus pneumoniae transformed with a novel Gram-positive lux transposon. Infect. Immun. 69, 3350-3358 (2001).
Visualization methods presented in this study could facilitate the study of bacterial infections and their treatment.
49. Ochs, H. D., Davis, S. D. & Wedgwood, R. J. Immunologic responses to bacteriophage [phi]X174 in immunodeficiency diseases. J. Clin. Invest. 50, 2559-2568 (1971).
This paper presents some of the initial experiments using phage to probe the human and mammalian immune systems.
50. Ochs, H. D., Nonoyama, S., Zhu, Q., Farrington, M. & Wedgwood, R. J. Regulation of antibody responses: the role of complement and adhesion molecules. Clin. Immunol. Immunopathol. 3, S33-S40 (1993).
51. Clark, L., Greenbaum, C., Jiang, J., Lernmark, Å. & Ochs, H. The antibody response to bacteriophage is linked to the lymphopenia gene in congenic BioBreeding rats. FEMS Immunol. Med. Microbiol. 32, 205-209 (2002).
52. Ching, Y -C., Davis, S. D. & Wedgwood, R. J. Antibody studies in hypogammaglobulinemia. J. Clin. Invest. 45, 1593-1600 (1966).
53. Jenne, S., Brepoels, K., Collen, D. & Jespers, L. High-resolution mapping of the B cell epitopes of staphylokinase in humans using negative selection of a phage-displayed antigen library. J. Immunol. 161, 3161-3168 (1998).
54. Bartlett, J. G. Antibiotic-associated diarrhea. N. Engl. J. Med. 346, 334-339 (2002).
55. Scholl, D., Rogers, S., Adhya, S. & Merril, C. Bacteriophage K1-5 encodes two different tail fiber proteins allowing it to infect and replicate on both K1 and K5 strains of E. coli . J. Virol. 75, 2509-2515 (2001).
Adaptations of the phage construct presented in this paper could provide a general approach for the extension of the bacterial host range of phage.
56. Scholl, D., Adhya, S. & Merril, C. R. Bacteriophage SP6 is closely related to phages K1-5, K5 and K1E but encodes a tail protein very similar to that of the distantly related P22. J. Bacteriol. 184, 2833-2836 (2002).
57. Sandmeier, H. Acquisition and rearrangement of sequence motifs in the evolution of bacteriophage tail fibres. Mol. Microbiol. 12, 343-350 (1994).
58. Liu, M. et al . Reverse transcriptase-mediated tropism switching in bordetella bacteriophage. Science 295, 2091-2094 (2002).
59. Moffatt, B. A. & Studier, F. W. Entry of bacteriophage T7 DNA into the cell and escape from host restriction. J. Bacteriol. 170, 2095-2105 (1988).
60. Hollon, T. Impossible vaccine tames Staphylococcus aureus . The Scientist 16, 24-28 (2002).
61. Gabig, M. et al . The cell surface protein Ag43 facilitates phage infection of Escherichia coli in the presence of bile salts and carbohydrates. Microbiology 148, 1533-1542 (2002).
62. Danese, P. N., Pratt, L. A., Dove, S. L. & Kolter, R. The outer membrane protein, antigen 43, mediates cell-to-cell interactions within Escherichia coli biofilms. Mol. Microbiol. 37, 424-432 (2000).
63. Colvin, M. G. Behavior of bacteriophage in body fluids and in exudates. J. Infect. Dis. 51, 527-541 (1932).
64. Calalb, G. Action de la bile sur bacteriophage et importance de cette action. Compt. Rend. Soc. De biol. (Paris) 92, 1442-1443 (1925).
65. Wagner, P. L. & Waldor, M. K. Bacteriophage control of bacterial virulence. Infect. Immun. 70, 3985-3993 (2002).
66. Altschul, S. F., Gish, W., Miller, W., Myers, E. W. & Lipman, D. J. Basic local alignment search tool. J. Mol. Biol. 215, 403-410 (1990).
67. Loessner, M. J., Rees, C. E. D., Steward, A. B. & Scherer, S. Construction of luciferase reporter bacteriophage A511::luxAB for rapid and sensitive detection of viable Listeria cells. Appl. Environ. Microbiol. 62, 1133-1140 (1996).
68. Carriere, C. J. et al . Conditionally replicating luciferase reporter phages: improved sensitivity for rapid detection and assessment of drug susceptibility of Mycobacterium tuberculosis . J. Clin. Microbiol. 35, 3232-3239 (1997).
69. Schuch, R., Nelson, D. & Fischetti, V. A. A bacteriolytic agent that detects and kills Bacillus anthracis . Nature 418, 884-889 (2002).
70. Lay, J. O. Jr MALDI-TOF mass spectrometry of bacteria. Mass Spectrom. Rev. 20, 172-194 (2001).
71. Van Baar, B. L. M. Characterization of bacteria by matrix-assisted laser desorption/ionisation and electrospray mass spectrometry. FEMS Microbiol. Rev. 24, 193-219 (2000).
72. Hamels, S. et al . Consensus PCR and microarray for diagnosis of the genus Staphylococcus species and methicillin resistance. BioTechniques 31, 1364-1366, 1368, 1370-1372 (2001).
73. Uhr, J. W., Finkelstein, M. S. & Baumann, J. B. Antibody formation: III. the primary and secondary antibody response to bacteriophage [psi]X 174 in guinea pigs. J. Exp. Med. 115, 655-670 (1962).
74. Lederberg, J. Smaller fleas...ad infinitum: therapeutic bacteriophage redux. Proc. Natl Acad. Sci. USA 93, 3167-3168 (1996).
This review stresses the need for additional research to facilitate the use of these viruses as safe and effective therapeutic antibacterial agents.
75. Knight, J. Superbugs reveal chink in armour. Nature 417, 477 (2002).
76. Kilman, S. FDA restricts antibiotic use in livestock to protect people. The Wall Street Journal D3 (12 September, 2002).
77. Merril, C. R. et al . Isolation of bacteriophages from commercial sera. In Vitro 8, 91-93 (1972).
78. Merril, C. R. Phage in human vaccines. Science 188, 8 (1975).
79. Bernhardt, T. G., Wang, I -N., Struck, D. K. & Young, R. A protein antibiotic in the phage Qb virion: diversity in lysis targets. Science 292, 2326-2329 (2001).
80. Nelson, D., Loomis, L. & Fischetti, V. A. Prevention and elimination of upper respiratory colonization of mice by group A streptococci by using a bacteriophage lytic enzyme. Proc. Natl Acad. Sci. USA 98, 4107-4112 (2001).
81. Gaeng, S., Scherer, S., Neve, H. & Loessner, M. J. Gene cloning and expression and secretion of Listeria monocytogenes bacteriophage-lytic enzymes in Lactococcus lactis . Appl. Environ. Microbiol. 66, 2951-2958 (2000).
82. Naidu, B. P. B. & Avari, C. R. Bacteriophage in the treatment of plague. Ind. J. Med. Res. 19, 737-748 (1932).
83. Boyd, E. F., Davis, B. M. & Hochhut, B. Bacteriophage-bacteriophage interactions in the evolution of pathogenic bacteria. Trends Microbiol. 9, 137-144 (2001).
Author Affiliation(s):
[1] Section on Biochemical Genetics, National Institute of Mental Health, National Institutes of Health, Bethesda, Maryland 20892, USA.
Email: merrilc@helix.nih.gov
Email: dscholl@helix.nih.gov
[2] Section of Developmental Genetics, National Cancer Institute, National Institutes of Health, Bethesda, Maryland 20892, USA.
Email: sadhya@helix.nih.gov
Author Bio(s):
Carl R. Merril is the chief of the Section on Biochemical Genetics at the National Institute of Mental Health (NIHM), National Institutes of Health (NIH). He has co-authored 225 articles, and 23 patents. His research ranges from basic and applied bacteriophage studies to the development of sensitive protein detection methods, including the silver stains. One of his publications concerning this methodology was declared a citation classic by the journal Current Contents as it earned more than 2,500 citations since its publication. In addition, two of his patents in this field have earned recognition as top money-makers for the Public Health Service (PHS), defined as a PHS-invented commercialized product that exceeds US $100,000 in annual sales. He has received a number of awards including the PHS Distinguished Service Medal and the Surgeon General’s Exemplary Service Medal.
Dean Scholl is a fellow in the Section on Biochemical Genetics at the NIMH, NIH. He has co-authored eight papers and three patents.
Sankar L. Adhya is the chief of the Section on Developmental Genetics, National Cancer Institute, NIH. He has co-authored more than 150 articles and 10 patents. He has received a number of awards, including election to the US National Academy of Sciences, the Indian Academy of Sciences and the American Academy of Microbiology.
DOI: 10.1038/nrd1111
Anthrax stopper
Travis, John
Science News
08-24-2002
SCIENCE NEWSThis Week
Viral enzyme detects, kills bacterium
Last fall, envelopes full of anthrax-causing spores killed 5 people, sickened about a dozen, and struck fear in millions. Researchers funded by the U.S. military have now developed an innovative way to detect and kill Bacillus anthracis, the bacterium that causes anthrax. Seeking help from nature, the researchers are using an enzyme produced by a bacteriophage, a virus that preys upon bacteria.
The enzyme, called lysin, prevented the death of most mice that the researchers had infected with a bacterial relative of B. anthracis, Raymond Schuch of Rockefeller University in New York and his colleagues there report in the Aug. 22 Nature. The investigators also used the enzyme to create a prototype handheld instrument that quickly detects the anthrax bacterium, even in its spore form.
"This is avery clever exploitation" of lysin, says biowarfare researcher Stephen Morse of Columbia University.
Bacteriophages, or phages, infect bacteria in order to reproduce inside. Once they do, phages use lysin to break apart their hosts cell walls so the new phages can infect other bacteria "They cause the [bacterium] to explode," says study coauthor Vincent A. Fischetti.
Discovered nearly a century ago, bacteriophages have long attracted the interest of physicians seeking to control bacterial infections. Antibiotics stole the spotlight from phage therapy for many decades, but there's renewed interest in the strategy, given the rise of antibiotic-resistant bacteria (SN: 6/1/96, p. 350; 6/3/00, p. 358).
Over the past few years, Fischetti and his colleagues have exploited the bacteria-- killing talent of phages in a different way. They've shown that lysin itself represents a new way to destroy bacteria. For example, they've successfully used lysin to treat animals infected with bacteria that cause strep throat and pneumonia in people (SN: 6/10/00, p. 376).
Fischetti's group recently turned its attention to potential biowarfare agents, starting with the anthrax bacterium. While conventional antibiotics can treat many strains of B. anthracis, there's concern that resistant strains could evolve or be created, says Fischetti.
He and his colleagues began working with a phage that infects the anthrax bacterium almost exclusively and identified the gene encoding its lysin. In test-tube experiments, the enzyme destroyed strains ofB. anthracis collected from around the world but left most other bacteria unscathed.
Next, the scientists tested the enzyme on mice infected with a strain of Bacillus cereus closely related to the anthrax bacterium. This strain serves as an initial testing ground for anthrax therapies because B. anthracis is so dangerous to work with. The B. cereus strain typically kills infected mice, but treatment with lysin saved up to 76 percent of infected animals, Fischetti's team reports.
The researchers now plan to test the enzyme against B. anthracis, first in rodents and then in a nonhuman primate. If those experiments prove successfull, physicians would then assess the safety of the viral protein in human volunteers. If lysin passes muster, the U.S. and other governments could then consider stockpiling the enzyme for any future anthrax attack
Fischetti's group also built a B. anthracis detector. The investigators mixed lysin with chemicals that emit a flash of light when exposed to a substance released by dead bacteria. They also added an agent that induces B. anthracis spores to germinate, making them susceptible to lysin. Finally, they engineered a handheld light meter to monitor this broth and found it could detect a signal produced by as few as 100 spores within an hour of adding them to the broth.
"It's an innovative and promising strategy," says Morse.
Copyright Science Service, Incorporated Aug
24, 2002

..............................................
The prospect for bacteriophage therapy in Western medicine.(Report)
Carl R. Merril, Dean Scholl, Sankar L. Adhya. Nature Reviews Drug Discovery. June 2003 v2 i6 p489(9).Author's Abstract:
Bacteriophage (phage) have been used for clinical applications since their initial discovery at the beginning of the twentieth century. However, they have never been subjected to the scrutiny -- in terms of the determination of efficacy and pharmacokinetics of therapeutic agents -- that is required in countries that enforce certification for marketed pharmaceuticals. There are a number of historical reasons for this deficiency, including the overshadowing discovery of the antibiotics. Nevertheless, present efforts to develop phage into reliable antibacterial agents have been substantially enhanced by knowledge gained concerning the genetics and physiology of phage in molecular detail during the past 50 years. Such efforts will be of importance given the emergence of antibiotic-resistant bacteria.
Full Text: COPYRIGHT 2003 Nature Publishing Group
Author(s): Carl R. Merril [1]; Dean Scholl [1]; Sankar L. Adhya [2]
The first widely used antibiotic, penicillin, was discovered 75 years ago. Since then, the production of antibiotics has grown into an industry with a market value estimated to exceed US $25 billion per year. Although antibiotics have saved countless lives, their widespread use has contributed to an increase in the incidence of antibiotic-resistant bacterial strains. For example, at the beginning of the antibiotic era Streptococcus pneumoniae was highly sensitive to penicillin, yet now, in some regions of the world, 25% of S. pneumoniae strains are resistant [1]. In addition, 70% of hospital-acquired bacterial infections in the United States are now resistant to one or more of the main antibiotics [2] and greater than 50% of clinical Staphylococcus aureus isolates in Japan are now multidrug resistant [3]. However, antibiotics are only one example of antibacterial entities that have arisen through the evolutionary competition between other species and bacteria. Another entity, the bacterial viruses (bacteriophage or PHAGE), might provide an alternative to fill the space created in the physician’s toolkit left by the dearth of new medicines to combat infections with antibiotic-resistant bacteria (Fig. 1).
The ability of phage to replicate exponentially and kill pathogenic strains of bacteria indicates that they should play a vital role in our armamentarium for the treatment of infectious diseases. In fact, such an application for phage was apparent to Felix d’Herelle after they were discovered by Twort in 1915 (Refs 4,5). d’Herelle was encouraged by his early experiments, in which he used phage to treat avian typhosis in chickens, shigella dysentery in rabbits and humans with bacillary dysentery. Following the reported successes of these experiments, d’Herelle travelled around the world stimulating basic and clinical phage research. Inspired by d’Herelle, the British medical officer Lieutenant Colonel Morison used phage for the prophylactic treatment of cholera epidemics in the Naogaon region of India from 1930 to 1935. In 1932, Morison reported few cholera deaths in the phage-treated Naogaon region, in contrast to the 474 deaths recorded in the Habiganj region which refused treatment [6, 7].
d’Herelle was also important in the establishment of a phage institute in Tbilisi, Soviet Georgia. This institute produced large quantities of phage for antibacterial therapy during and immediately following the Second World War and the institute is still actively pursuing phage therapy applications. Applications of phage as pursued in the Soviet Union (as well as Poland) have been extensively reviewed [8, 9]. The authors of these reviews noted that the details of phage dosages are presented primarily as qualitative data and that clinical criteria were generally reported in a ’sketchy’ manner. For these reasons, most of the studies from Eastern Europe will not meet the present standards for pharmaceutical approval in countries that require certification based on the results of efficacy and pharmacokinetic studies in animals and humans.
There was also an interest, in the 1920s and 1930s, in phage therapy in the United States. The large pharmaceutical company Eli Lilly & Co. sold ’Staphylo jel’, and other phage ’jel’ labelled products, for the treatment of Streptococcus spp. and colon bacilli infections. E. R. Squibb & Sons and the Swan-Myers division of Abbott Laboratories marketed a bacteriophage filtrate preparation for Staphylococcus spp., and combined bacteriophage filtrate preparations for Staphylococcus spp. and colon bacilli, respectively [10]. Despite this initial enthusiasm for phage products, clinical failures, theoretical concerns and the overshadowing development of antibiotics resulted in the abandonment of phage therapy in the United States and much of Western Europe [10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20](TIMELINE).
Re-examination of potential efficacy
Despite the chequered history of phage therapy, concerns over the increased incidence of antibiotic resistance has led investigators to examine the possibility of developing phage therapy into a reliable clinical tool. In one recently published animal study, a vancomycin-resistant Enterococcus faecium strain was used to induce a fatal bacteraemia (within 48 hours) in mice. Treatment with a single intraperitoneal injection of phage 45 minutes after the bacterial challenge was sufficient to rescue 100% of the animals, and even when treatment was delayed until the animals were moribund, phage administration was able to rescue 50% of the mice [21]. Similar results have been obtained using phage to treat animals infected with methicillin-resistant S. aureus [22]. In addition, phage have been used to treat Acinetobacter baumanii or Pseudomonas aeruginosa and animals with local and systemic disease caused by Vibrio vulnificus [23, 24].
Phages are also capable of treating antibiotic-resistant intracellular pathogens. Broxmeyer et al . [25] have demonstrated that it is possible to use Mycobacterium smegmatis , an avirulent mycobacterium, as a vector to deliver the LYTIC PHAGE TM4 to treat intracellular mycobacterium infections (with either Mycobacterium avium or Mycobacterium tuberculosis ) in macrophages. Phages have also been effective in the treatment of non-systemic infections, such as gastrointestinal infections caused by enteropathogenic strains of Escherichia coli in calves, pigs and lambs and ileocecitis caused by Clostridium difficile in hamsters [26, 27, 28, 29]. Phages have also been shown to be effective in preventing the destruction of skin grafts by P. aeruginosa [30]. Terrestrial animals are not the only candidates for phage therapy, as recent studies have shown that phage can be used to treat bacterial diseases of fish in aquiculture [31], bacterial blight of geranium [32] and bacterial spot on tomatoes [33].

Phage pharmacokinetics
Although phage therapy has a long history, pharmacokinetic data are still rudimentary. Most clinical applications of phage therapy have relied on the oral administration of phage preparations. This choice offers the possibility of reducing side effects from contaminants, including ENDOTOXINS and EXOTOXINS, but it might not provide the most effective therapeutic regimen(s) [34]. Some early practitioners of phage therapy recognized the need for pharmacokinetic information. The first effort to obtain such data in 1921 led to the observation that phage injected into the circulatory system of rabbits could still be found in the spleen long after the elimination of phage from other organs or the blood [35]. This finding was corroborated by both qualitative and quantitative experiments, in which a decrease in phage titre in the blood of mice injected with a Staphylococcus phage (a decrease of four orders of magnitude of phage titres was observed 5 minutes after intravenous injection, and by seven logs two hours later) was attributed to elimination by the reticulo-endothelial system (RES) [17, 36].
The relative roles of the liver and spleen in this process were determined by using 51 Cr-labelled phage. In these experiments the liver phagocytosed more than 99% of the phage in the circulatory system and inactivated the phage at a higher rate than the spleen [37]. Antibodies associated with the ADAPTIVE IMMUNE SYSTEM were not involved in this process, as demonstrated by experiments using germ-free mice that had no detectable antibodies to the phage strain used. Systemically administered phages were rapidly eliminated from the circulation of the germ-free mice. Furthermore, these quantitative experiments demonstrated that the oral administration of phage was not an effective method for delivery to systemic sites [34] (Fig. 2). Recognition that the RES can remove a significant proportion of administered phage led to the development of a serial passage selection method to isolate phage mutants with a greater capacity to remain in the circulatory system of the mouse. These ’long-circulating’ phage mutants also proved to be more effective therapeutically [38].
In studying the pharmacokinetics of phage it should be noted that phage DNA, like any other foreign DNA, can get into mammalian cells and, on rare occasions, into chromosomes [39, 40, 41]. There have also been reports of phage-induced enzyme activity in mammalian cells, albeit at low levels, following exposure to phage or phage DNA [42, 43]. Although there are efforts underway to enhance the capability of phage to serve as vectors for targeted gene delivery in mammalian cells [44], there is evidence that in the natural setting such effects are normally minimal: phages are, for example, associated with bacteria in our colon, nose, throat and skin throughout our life span.
For nearly all pharmacological agents, information on drug distribution and clearance would be sufficient for pharmacokinetic studies. However, unlike most pharmaceuticals, phage can replicate exponentially. The exploitation of phage as antibacterial therapeutics requires knowledge of three dynamic components: the infected human, the infecting bacteria and the phage, and their complex interactions. Of these three dynamic components, two of them -- the bacteria and the phage -- are capable of exponential growth during the course of an infection and its treatment. Given this situation, it is crucial to ensure that the phage titres employed are sufficient for a successful therapeutic outcome (Fig. 3). To explore such parameters, Smith and Huggins used two experimental models, one in which mice were infected intracerebrally with E. coli K1 and another in which they were infected intramuscularly. Phage was administered intramuscularly in both of these studies. The phage levels were found to be highest in the infected tissues and they fell as the bacterial levels in the infected tissue decreased.
These results corroborated the earlier finding of Dubos et al . [18] that mice infected intracerebrally with Shigella dysenteriae were rescued by administering phage into the peritoneal cavity [45]. In these experiments, the survival of untreated animals was 3.6%, whereas the survival of phage-treated animals was 72%. In addition, phage levels were observed to increase at the site of the infection -- the brain -- whereas the blood levels of phage seemed to be a "reflection of the events occurring in the brain". In uninfected control animals injected with phage, phage levels in the blood were compatible with the dilution of the phage in the total blood volume of the mouse. These researchers also showed that heat-inactivated phage provided no protective effects unless given days before the bacterial infection, and suggested that the protective effect of such heat-inactivated phage might result from the activation of antibacterial immunity by bacterial products present in the phage LYSATE.
Levin and Bull [46], and Payne and Jansen [47], have developed formal mathematical models on the basis of data from the Smith and Huggins [26] study. The Payne and Jansen [47] model included terms for the loss of phage resulting from interaction with mammalian systems, such as the RES. Their analysis with this model corroborated the suggestion by Alinsky et al . [8] that antibiotic and phage therapies might not be synergistic. Although such models are important for pharmacological planning, present efforts are based on limited datasets. Recently developed methods of visualizing bacterial infections in live animals using bioluminescent strains of bacteria might help in such pharmacokinetic studies [48]. This method uses a high sensitivity charge-coupled device camera to monitor bacteria in live mice. The bacteria are made bioluminescent by incorporating a luciferase transposon cassette into their genome. As it is feasible to incorporate luciferase transposon cassettes into phage genomes, it should also be possible to follow phage interactions with bacterial infections in vivo .
Phage immunogenicity
Phage immunogenicity is important for two reasons: first, because of potential adverse reactions, such as anaphylactic shock, and second, because of its effects on the pharmacokinetics of phage therapy. When phage are first used, some behave as NEO-ANTIGENS, as there are no pre-existing antibodies for these phage. This feature, along with the lack of apparent side effects, has permitted the use of phage [phi]X174 as a probe of human and animal immune sytems [49, 50, 51]. Despite the apparent lack of antibodies to phage that present as neo-antigens they still interact with the innate immune system, as demonstrated by the rapid loss of phage injected into the circulatory system of germ-free mice [34] and the capacity of the liver to phagocytose more than 99% of administered phage within 30 minutes of inoculation [37]. It is important to note that not all phage present as neo-antigens, as Kucharewica-Krukowska and Slopek noted in a study in which 11% of their healthy controls and 23% of their patients had antibodies against a Staphylococcus phage strain before administration of phage therapy [45].
If a particular phage strain were used repeatedly as an therapeutic antibacterial agent, in addition to the interactions with the innate immune system, the adaptive immune system would be stimulated and result in the production of antibodies. Such activation of the adaptive immune system relies on somatic mutations and clonal expansion of T and B cells, which can take at least three to five days. In normal individuals injected with the highly immunogenic phage [phi]X174, the phage is normally cleared within three days and a primary immunoglobulin M (IgM) response can be observed that peaks two weeks after the initial injection or immunization. If another injection is made six weeks later, the IgM and IgG antibody titres increase and peak within one week of the second injection; subsequent phage injections result in further increases in the IgG titres [50]. Patients with severe combined immune deficiency (SCID), which is characterized by the absence of both B and T cell functions, display a prolonged period for the clearance of phage, with phage present up to four to six weeks after the initial injection. In addition, SCID patients do not develop detectable antibody responses to phage, even after repeated injections. Ochs and his colleagues have also found that although [phi]X174 phage is a potent antigen, it causes no recognized toxic effects in man [49, 52].
Similar findings were reported for the phage ENB6 used to treat mice infected with vancomycin-resistant Enterococcus [21]. To determine the immunogenicity of this phage, mice were given monthly injections. After the third in a series of five monthly injections, the titres of IgG and IgM increased 3,800-fold and fivefold, respectively, above background. The IgG levels did not change substantially after the third phage injection. No anaphylactic reactions, changes in core body temperature or other adverse events were observed in the mice over the course of these multiple injections of phage [21]. It might be possible to develop phage that are less antigenic by using phage-displaying peptide libraries or affinity matrixes made up of antibodies from human serum. This type of approach has been initiated to decrease the immunogenicity of therapeutically important enzymes [53].
Bacterial host specificity of phage
The bacterial host range of phage is generally narrower than that found in the antibiotics that have been selected for clinical applications. Most phage are specific for one species of bacteria and many are only able to lyse specific strains within a species. This limited host range can be advantageous, in principle, as phage therapy should result in less harm to the normal body flora and ecology than commonly used antibiotics, which often disrupt the normal gastrointestinal flora and result in opportunistic secondary infections by organisms such as C. difficile [54]. The potential clinical disadvantages associated with the narrow host range of most phage strains can be addressed through the development of a large collection of well-characterized phage for a broad range of pathogens, and methods to rapidly determine which of the phage strains in the collection will be effective for any given infection.
Ideally, broad-host-range phage should be selected for therapeutic applications. However, if such phage strains cannot be found, present molecular techniques can be used to enhance the host range of some phage strains. For example, it has been found that coliphage K1-5 is a ’dual’ specificity phage that encodes two different tail proteins; this allows it to attack and replicate in both K1 and K5 strains of E. coli [55]. One tail protein found on phage K1-5 is a lyase protein, similar to that of phage K5 (specific for the K5 polysaccharide capsule), and a second tail protein found on this phage is an ENDOSIALIDASE similar to a tail protein found in phage K1E (specific for the K1 polysaccharide capsule). In addition, the genomic region encoding these proteins is almost identical to the genomic construct found in the salmonella phage SP6, which codes for a protein that binds to the salmonella O-antigen [56]. The observation of a similar tail genome motif in both the salmonella phage SP6 and the coliphages K1E, K5 and K1-5 indicates that this genomic construct might serve in the development of a modular phage platform that could operate over a wide bacterial host range.
Other mechanisms have been found that permit expansion of the bacterial host range of phage. These include the site-specific recombination systems that permit phage to switch between alternative tail fibre proteins [57] and the use of a reverse transcriptase, possessed by a Bordetella phage, to generate variation in its tail fibre proteins [58]. Such expanded host-range ’platform’ phage would provide for versatility and save time and effort compared with that required for the development of completely new phages for each bacterial strain.
Other factors can affect host specificity. For example, bacterial restriction/modification systems might limit the host range of some phage. This problem could be addressed, in principle, by engineering phages with genomes that do not contain restriction sites recognized by the non-permissive host. Alternatively, phages could be produced in bacterial strains that provide DNA modification(s) that allow the phage to escape restriction in the targeted strain of bacteria. Another approach would be to incorporate genes into the phage genome that facilitate inhibition of bacterial restriction/modification enzymes, as exemplified by the mechanism used by the phage T7 which encodes an antirestriction enzyme [59]. A construct containing such an antirestriction gene might be adapted for use in other phage strains, or it might be possible to modify T7 phage to expand its bacterial host range for E. coli infections.
Phage growth: in vitro versus in vivo
In addition to the factors addressed above, bacteria grown with standard laboratory protocols can behave differently in the milieu of an infection. Bacteria possess feedback mechanisms that can alter their gene expression in response to changing environmental conditions. Such variations in gene expression can affect phage susceptibility. For example, Karakawa noted that S. aureus rarely expresses the capsular polysaccharides found in clinical isolates when the bacteria are grown in the laboratory [60]. Given the possibility for such changes in the bacterial capsule, phage discovered using bacteria grown in vitro might not be able to multiply in an infected animal. Recently, it has been reported that phage that infected certain strains of E. coli that did not express the cell surface protein Ag43 in standard laboratory growth media can be inhibited by concentrations of bile salts similar to that found in the gastrointestinal tract [61]. In this case, the bile salts might affect the expression of the Ag43 protein, which has been shown to be a phase -variable protein whose expression is associated with E. coli BIOFILM formation [62].
In addition, different in vitro and in vivo bacterial densities can be important [47]. Variations in phage physiology also are important, as some phage infections cause the host bacteria to release lysins that result in the destruction of bacteria not directly infected by the phage ([Box 1] and Fig. 4). In the early phage literature, there are reports of body fluids (for example, serum, pus, ascites fluids, cerebrospinal fluid, urine and bile) that inhibit the infectivity of phage that were active in vitro against typhoid, colon bacilli and staphylococci [63, 64]. Some of these effects might have resulted from alterations of bacterial physiology.
Detrimental phage genes
Some phage strains, the lytic phage, kill bacteria, whereas others -- LYSOGENIC or temperate phage -- have a dual life style: they can either kill and lyse their bacterial host or become quiescent by integrating their genome into their bacterial host chromosome. Some lysogenic phage encode toxins or factors that enhance bacterial pathogenesis (Table 1). Phage can also contribute, through transduction, to the transmission of antibiotic-resistance genes [65]. It is essential that phage considered for therapeutic applications be screened for toxin genes, either biochemically or by sequencing their DNA. The presence of toxin, antibiotic resistance genes, and genes that increase bacterial pathenogenicity, can be checked by searching phage genomes against GenBank online using the Basic Local Alignment Search Tool (BLAST) [66] and other similar programs. Success cannot be assumed as we are still in the discovery stage of such detrimental genes. The usefulness of bioinformatic analysis will increase as knowledge of these potential deleterious genes accumulates.
Selection of therapeutic phage strains
The narrow host range of most phage strains dictates the need for the rapid determination of bacterial susceptibility. The determination of suitable therapeutic phage strain(s) using traditional procedures can take days to accomplish, limiting the use of phage therapy to slowly progressing infections. However, recent methods have been developed that permit the identification of both the infectious agent and a suitable phage strain within a day or less.
One such approach uses of phage that contain reporter genes, such as luciferase [67, 68]. For example, a collection of phage strains, each encoding luciferase protein, could be individually placed in a multi-well plate. When a clinical sample, such as urine or sputum, is added to the wells, light will be emitted and detected in those wells that contain a phage strain that successfully infects the bacteria in the clinical specimen. Such light emission would serve to identify both bacterial strains and the phage strains that could be used against them. This test could be performed in hours, instead of the days that traditional culture methods require. This approach has been used to detect Listeria contamination in foods [67] and in an inexpensive and rapid diagnostic test for tuberculosis [68]. Alternatively, similar results can be achieved by using phage that do not have such marker genes, by placing luciferin and luciferase in the phage/bacterial incubation mixture in each of the wells of the multi-well plate. The lysis of bacterial strains by a phage strain in any of the wells will result in the discharge of adenylate kinase into the well, which will convert the ADP in the reaction mix to ATP. As the luciferin/luciferase system can utilize the ATP for light emission, lysis will serve to identify phage susceptibility without the need to genetically engineer the phage with a luciferase reporter gene [69].
Another method for the rapid identification of bacterial strains could be provided by mass spectrometry (MS). Mass fragment ’fingerprints’ of lipid, protein and nucleic acid bacterial components are used at present for rapid strain identification [70, 71]. It might also be possible to use this approach to determine whether bacteria are susceptible to a particular phage strain. However, such information is not available at present and it might be impractical to gain sufficient knowledge of bacterial mass fingerprints to determine which phage strains to use therapeutically for a bacterial host responsible for an infectious disease. Alternatively, phage gene products might provide for the development of markers for both bacterial identification and as an indicator of phage susceptibility. In this approach, one could use MS by placing a clinical sample in growth media to amplify the infecting bacteria followed by exposure to selected ’therapeutic’ phage strains. If the bacteria were susceptible to the phage, MS would detect signature fragments of phage proteins that are expressed only when infection of the bacteria occurs by a specific phage. Such ’signature’ fragments, that are not part of the phage virion, would be generated from phage: RNA polymerase, regulatory protein or lytic enzymes.
DNA microarray technologies also offer possibilities for determining bacterial strains in disease states and possibly the phage strains that might be used therapeutically. DNA microarrays, in conjunction with polymerase chain reaction, are now being developed for the rapid diagnosis of bacterial strains and antibiotic susceptibility [72]. In principle, it might be possible to develop such methods for the determination of bacterial strains and their phage susceptibility.

Development and preparation of phage
In addition to biological factors, phage preparative methods are crucial for the development of reliable phage therapeutics. Early therapeutic applications used impure phage preparations with deleterious clinical effects ([Box 2]). Contamination of phage preparations can result in increased morbidity or, in some cases, mortality. For example, in a recently published study, intraperitoneal inoculation of mice with filter-sterilized phage lysates produced reactions associated with endotoxin levels that ranged from mild (ruffled fur) to death [38]. Adequate purification, for example, by physical and/or biochemical methods, must be adopted for the production of toxin-free, clinical-grade phage preparations with long-term storage stability [38, 73]. Phage prepared in this manner have been administered to animals without any noticeable ill effects and Ochs et al . have used such purified phage in their human protocols [49].
In developing phage purification procedures, testing for adverse effects should not be limited to observation with healthy animals. Individuals that are under stress can have a lowered tolerance to endo- and exotoxins. In a recent mouse bacteraemia study, a lower survival rate was observed in a ’control experiment’ in which a phage strain, known to be inactive against the bacterial strain being used at the LD50 level, was administered to the infected mice. Although the highest doses of this phage preparation produced no apparent adverse effects in healthy uninfected animals, an increased mortality was observed in the bacteraemia-stressed mice. This increased mortality was phage-dose dependent, indicating that stressed animals are more sensitive to the phage itself, or to the trace amounts of endo- and exotoxins present in the phage preparations, than normal animals [21]. This example provides additional evidence for the need for highly purified phage preparations for therapeutic applications.
It should also be noted that bacteriostatic or bacteriocidal agents, used to ensure that no active bacteria are present in phage preparations, can also be detrimental. The association between ’weak’ phage preparations and the presence of organomercury compounds was made in a 1932 study of commercial phage preparations from a large US pharmaceutical company [10].
Future prospects
Although results from animal experiments are encouraging, continuing research will be needed to develop phage therapy for the treatment of human infectious diseases. These efforts should include studies of phage genomics, pharmacokinetics and efficacy in animal models of infectious diseases. In addition, phage chosen for therapeutic applications will need to be screened to reduce the chance that they carry genes encoding toxins, or factors that enhance bacterial pathogenicity. Phage growth, purification and storage protocols are needed to assure therapeutic efficacy and to reduce the possibility of contamination of pharmaceutical preparations by toxins and bacterial debris. Furthermore, the narrow host range of most phage strains requires the development of rapid methods for the determination of appropriate phage strains for use in specific infections.
Development of therapeutic phage could provide some relief from the growing threat from the emerging antibiotic-resistant bacterial strains and, as Lederberg suggested, treatments for epidemics such as cholera in refugee camps [74]. In addition, the narrow host range of phage could be better suited than presently employed antibiotics to a number of clinical applications. For example, the lack of genetic variability in antibiotic-resistant bacteria suggests that the resulting pathogenic bacteria might offer ideal targets for phage therapy. Only 10 strains of Pneumococcus are associated with 75% of the cases of antibiotic-resistant childhood pneumonia, and one-half of these cases are caused by the single strain ’Spain 23-E’. Herminia de Lencastre obtained similar results in a study of methicillin-resistant S. aureus , in which only five strains of methicillin-resistant S. aureus were found in 70% of 3,000 clinical isolates from 14 countries [75]. The narrow host range of phage should also reduce the disturbance of the complex bacterial ecological systems associated with the human gastrointestinal system. Applications of phage to treat infections could eliminate the IATROGENIC effects of antibiotics, such as the antibiotic-related diarrhoea diseases that range from ’nuisance’ diarrhoea to colitis associated with C. difficile infections [55].
Phage, with their narrow host range, could also prove useful in treating bacterial infections in agricultural applications without disturbing larger ecological systems, as is often the problem with antibiotics [74]. This suggestion is strengthened by the recent observations that many antibiotic-resistant bacterial strains are arising through clonal selection. In recognition of this growing problem, the FDA recently announced that it is re-evaluating livestock antibiotics, and it is now requiring manufacturers of proposed livestock antibiotics to determine whether these proposed antibiotics will be associated with the emergence of pathogenic organisms with resistance to drugs presently in use for the treatment of human diseases [76].
In regard to concerns over regulatory agency approval, it should be noted that phage have been used successfully as a means to probe immune-deficiency diseases in human studies for the past three decades [49, 50]. In addition, some vaccines were found, in the 1970s, to be contaminated with phage. An executive order was issued to permit the continued use of these contaminated vaccines [77, 78]. We should also recognize that we are normally in contact with phage throughout our lifetime, with the complex interactions of bacteria and phage in our colon, upper respiratory system and on our skin. In fact, many present phage collections were derived from human waste.
It is clear from recent experiments that phage therapy has the potential to rescue animals infected with antibiotic-resistant bacterial stains [22, 21]. We now also have much of the knowledge needed to develop phage into reliable therapeutic preparations. Whether we embark on efforts needed to develop therapeutic phage for human infections depends in part on our need to obtain relief from the growing threat of emerging antibiotic-resistant bacterial strains and our will to accomplish this task.

Definition List:
ADAPTIVE IMMUNE SYSTEM: The arm of the immune system that mounts an antigen-specific immune response as the result of the clonal selection of antigen-specific lymphocytes. Such lymphocytes produce antibodies that react with the antigen. The adaptive immune responses differ from the innate and non-adaptive immune system, which does not depend on clonal selection of antigen-specific lymphocytes.
BIOFILM: A structure made up of a community of bacteria composed of microcolonies and water channels that survives at a liquid interface. Such biofilms play a role in the pathogenic effects of bacterial infections associated with gingivitis, colitis, vaginitis, urethritis, conjunctivitis and otitis.
ENDOTOXINS: Components of bacterial cells that are usually associated with the lipopolysaccharide components of the outer layer of Gram-negative bacterial cell walls that are toxic (to mammals). Endotoxins are released in large quantities upon lysis of Gram-negative bacterial cells.
ENDOSIALIDASES: Enzymes that cleave at the sialic acid residue sites of the complex oligosaccharides associated with the protective capsule of many bacterial strains.
EXOTOXINS: A broad class of factors released by pathogenic bacteria that can harm infected mammals. Examples of such exotoxins are botulism toxin (Clostridium botulinum ), streptolysins (Streptococcus pyogenes ) and diphtheria toxin (Corynebacterium diptheriae ).
IATROGENIC: An effect that is induced in a patient by a physician’s activity or therapy; such effects often occur as complications of treatments for infectious diseases.
LD50 : The amount of a substance that causes the death of 50% of test subjects.
LYSATE: The colloidal bacterial growth media remaining after phage replicate and kill the host cells. Lysates contain phage progeny, bacterial cell wall debris and, often, internal cellular components (for example, proteins, nucleic acids, small molecules and so on).
LYSOGENIC PHAGE: Phage that are capable of integrating their genome (that is, lysogenize) into the host chromosome. Such phages often mediate horizontal gene transfer (transduction) between bacterial strains. Most lysogenic phage can also go through a lytic cycle to produce more phage, often after induction (from some environmental factor).
LYTIC PHAGE: Phage that infect bacterial cells to replicate and then lyse the bacterial host.
NEO-ANTIGEN: An antigen for which animals or humans being studied have no pre-existing antibodies. The phage [phi]X174, which is highly immunogenic, has served as such a neo-antigen in studies of human antibody responses, as most humans have no pre-existing antibodies to this phage.
PHAGE: Bacterial viruses. The term phage is used as both singular and plural when referring to phage(s) that is/are member(s) of a single phage strain. However, when referring to phage in more than one strain the plural is phages.
PHAGE PLAQUE: The lesion formed when a phage particle is applied to a film of a susceptible bacterial strain that is growing on an agar surface. The lesion results from the infection of a bacterial cell by a phage particle, followed by the production of phage progeny and their release by lysis, followed by the infection and lysis of additional bacterial cells in the vicinity of the initial infection.
Web Link(s):
DATABASES
Online Mendelian Inheritance in Man
Severe combined immunodeficiency: http://www.ncbi.nlm.nih.gov/htbin-post/Omim/dispmim?102700
FURTHER INFORMATION
Encyclopedia of Life Sciences
Bacteriophages: http://www.els.net/els/FDA/default.asp?id=25CA4A8E-4CC9-4DCE-9E33-D5DD1D5A2AE2
bacteriophages in industry: http://www.els.net/els/FDA/default.asp?id=5CF03976-9CBE-4DCB-9A53-D4CBFA9BD344
phage display technologies: http://www.els.net/els/FDA/default.asp?id=CED7B675-3979-43EF-BB87-8EE22D7BE08C
Genomes of the T4-like Phages: http://phage.bioc.tulane.edu/
Phage Ecology and Evolutionary Biology: http://www.mansfield.ohio-state.edu/~sabedon/
Phage Page: http://www.mbio.ncsu.edu/esm/phage/phage.html
Phage Therapy: http://www.evergreen.edu/phage/phagetherapy.html
Therapeutic uses of phage: http://surfer.iitd.pan.wroc.pl/phages/phages.html
Box 1 | Therapeutic use of phage products
Phage gene products might also serve as therapeutic agents. Although such applications lack the exponential growth capacity of phage, they could still be highly effective. For example, the small-genome phages [phi]X174 and Q[beta] encode polypeptides that could be developed into a new class of antibiotics, as they interfere with bacterial cell wall biosynthesis [79]. Such inhibition results in bacterial lysis. Similarly, phage-encoded endolysins that disrupt the peptidoglycan matrix of the bacterial cell wall, and phage-encoded holins that permeabilize bacterial membranes, can also serve as effective antibacterial agents. A phage lysin, specific for streptococci groups A, C and E, has been used to treat experimental upper respiratory infections in mice [80]. Such lysins should be less disruptive than most antibiotic treatments as they have little, if any, effect on other commensal organisms in the oral and upper respiratory tract. In another example, the [gamma] phage of Bacillus anthracis encodes a lysin that proved to be effective in rescuing mice infected with Bacillus cereus , a bacterial strain closely related to B. anthracis [69]. No resistant B. cereus strains were detected following such treatment. In addition, phage lysin genes have been incorporated into bacterial genomes for prophylactic applications. Gaeng et al . [81] developed such a bacterial strain to secrete the functional phage lysin enzymes Ply511 and Ply118 to reduce Listeria monocytogenes contamination in dairy cheese production starter cultures [81]. These phage lysins can also be used diagnostically. For example, when PlyG lysin destroys B. anthracis , ATP is released, which, in conjunction with the luciferin/luciferase system, results in the emission of light that can also be used to rapidly detect bacilli and their germinating spores. This system was able to detect as few as 100 spores [69].
Box 2 | Therapeutic failure that might have resulted from impure phage
Some of the early clinical therapeutic failures might have been due to inadequate purification of the phage preparations. In one such example, reported in 1932, a phage strain was found that seemed to be promising as a therapeutic agent as it could lyse cultures of plague (Yersinia pestis ) grown in broth media in less than 2 hours. However, when this phage strain, purified solely by filtration, was injected into rabbits experimentally infected with Y. pestis , the mortality increased to levels above those found in infected rabbits that were not treated with phage. Furthermore, when this phage preparation was used to treat 33 human patients, they all died. The mortality from plague is normally 60-90% [82].
Caption(s):
Illustration 1: Timeline | Highlights in the development of phage as a potential therapeutic agent for bacterial infections [see PDF for image]
Figure 1: Electron micrograph of phage. [see PDF for image]
This is an Escherichia coli phage. Phage can range from filamentous to spherical structures. However, many of them have a distinct head, containing their DNA, and a tail-like structure that can bind to bacterial receptors.
Figure 2: Systemic distribution of phage following intravenous and oral administration of phage. [see PDF for image]
These experiments demonstrate that oral administration is not an effective method for the delivery of phage to systemic sites as the blood and tissues levels were seven to eight orders of magnitude lower with oral administration than those achieved by systemic administration of phage. pfu, plaque-forming units.
Figure 3: The effect of therapeutic phage concentration on morbidity and mortality. [see PDF for image]
When phage are used to treat a systemic bacterial infection, the concentration of phage administered must be adequate to kill the infecting bacteria before they can kill the mammalian host. This point is illustrated in the data, from a study using phage to treat bacteraemic mice infected with 109 colony-forming units (cfu) of vancomycin-resistant Enterococcus faecium [21]. This concentration of bacteria normally results in death within 48 hours. Each bar represents a single mouse, and all but the two control mice (injected with buffer rather than bacteria, represented by the pink bars) were infected with 109 cfu of bacteria. The phage concentrations administered 45 minutes after the bacterial infection are depicted in the key. The mice in the last group (red bars) did not receive phage therapy. The state of health scale is a non-parametric scale in which: 5 = normal; 4 = decreased activity and ruffled fur; 3 = lethargy, ruffled fur and hunchback posture; 2 = hunchback posture and partially closed eyes with exudates; 1 = moribund; and 0 = death. pfu, plaque-forming units.
Figure 4: Phage plaques on a bacterial ’lawn’. [see PDF for image]
The PHAGE PLAQUES illustrated on this plate display a mixture of morphologies, which reflect the different phage strains applied to this bacterial plate. Some of the phage produce small clear plaques, whereas other phage strains that produce lysins have a clear centre zone surrounded by a spreading zone of killing.
Table: Phages that carry toxin genes and their gene products [83] [see PDF for image]
References
1. Thornsberry, C. et al . Regional trends in antimicrobial resistance among clinical isolates of Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis in the United States: results from the TRUST Surveillance Program, 1999-2000. Clin. Infect. Dis. 34, S4-S16 (2002).
2. National Center for Infectious Diseases. Campaign to prevent antimicrobial resistance in healthcare settings. Centers for Disease Control and Prevention [online] (cited 30 Sep 2002) <http://www.cdc.gov/drugresistance/healthcare/problem.htm> (2002).
3. Hashimoto, H. Drug resistance of methicillin-resistant Staphylococcus aureus (MRSA) in Japan until 1993. Jpn J. Antibiot. 47, 575-584 (1994).
4. Twort, F. W. An investigation on the nature of ultra-microscopic viruses. Lancet 2, 1241-1243 (1915).
This paper presents the original discovery of bacterial viruses.
5. d’Herelle, F. The Bacteriophage and its Behavior 490-541 (Williams & Wilkins, Baltimore, Maryland, 1926).
Although much of the material in this book is dated, it still contains observations of interest.
6. Summers, W. C. Felix d’Herelle and the origins of Molecular Biology 125-144 (Yale University Press, New Haven and London, 2001).
7. Summers, W. C. Bacteriophage therapy. Annu. Rev. Microbiol. 55, 437-451 (2001).
8. Alinsky, J., Iczkowski, K., Rapoport, A., & Troitsky, N. Bacteriophages show promise as antimicrobial agents. J. Infect. 16, 5-15 (1998).
This and the following article present an overall review of phage therapy efforts in Poland and the Soviet Union.
9. Sulakvelidze, A., Alavidze, Z. & Morris, J. G. Jr Bacteriophage therapy. Antimicrob. Agents Chemother. 45, 649-659 (2001).
10. Straub, M. E. & Applebaum, M. Studies on commercial bacteriophage products. JAMA 100, 110-113 (1933).
Insights into the problems associated with pharmaceutical phage preparations.
11. Larkum, N. W. Bacteriophage in clinical medicine. J. Lab. Clin. Med. 17, 675-680 (1932).
12. Van Helvoort, T. Bacteriological and physiological research styles in the early controversy on the nature of the bacteriophage phenomenon. Med. Hist. 36, 243-270 (1992).
13. Randall-Hazelbauer, L. & Schwartz, M. Isolation of the bacteriophage [lambda] receptor from Escherichia coli . J. Bacteriol. 116, 1436-1446 (1973).
14. Eaton, M. D. & Bayne-Jones, S. Bacteriophage therapy. JAMA 103, 1769-1776, 1847-1853 & 1934-1939 (1934).
15. Ho, K. Bacteriophage therapy for bacterial infections. Perspect. Biol. Med. 44, 1-16 (2001).
16. Barrow, P. A. & Soothill, J. S. Bacteriophage therapy and prophylaxis: rediscovery and renewed assessment of potential. Trends Microbiol. 5, 268-271 (1997)
17. Evans, A. C. Inactivation of antistreptococcus bacteriophage by animal fluids. Public Health Rep. 48, 411-426 (1933).
18. Dubos, R. J., Straus, J. H. & Pierce, C. The multiplication of bacteriophage in vivo and its protective effects against experimental infection with Shigella dysenteria . J. Exp. Med. 20, 161-168 (1943).
This paper presents crucial experiments designed to explore the mechanisms underlying the therapeutic effects observed when using phage to treat a systemic bacterial infection.
19. Asheshov, I. N., Wilson, J. & Topley, W. W. C. The effect of an anti-vi bacteriophage on typhoid infection in mice. Lancet 319-320 (1937).
20. Stent, G. S. Molecular Biology of Bacterial Viruses (W. H. Freeman, San Francisco, 1963).
Essential information for those interested in phage and their applications, and provides insights into theories concerning phage therapy failures.
21. Biswas, B. et al . Bacteriophage therapy rescues mice bacteremic from a clinical isolate of vancomycin-resistant Enterococcus faecium . Infect. Immun. 70, 204-210 (2002).
In addition to a demonstration of the effectiveness of phage therapy for treatment of animals infected with antibiotic resistant bacteria, the experiments in this study also show that the rescue of infected animals is directly dependent on phage function.
22. Matsuzaki, S. et al . Experimental protection of mice against lethal Staphylococcus aureus infection by novel bacteriophage MR11. J. Infect. Dis. 187, 613-624 (2003).
The animal experiments described in this paper provide evidence that phage could provide an alternate therapeutic approach for the treatment of a serious antibiotic-resistant bacterial infection.
23. Soothill, J. S. Treatment of experimental infections of mice with bacteriophages. J. Med. Microbiol. 37, 258-262 (1992).
24. Cerveny, K. E, Depaola, A., Duckworth, D. H & Gulig, P. A. Phage therapy of local and systemic disease caused by Vibrio vulnificus in iron-dextran-treated mice. Infect. Immun. 70, 6251-6262 (2002).
25. Broxmeyer, L. et al . Killing of Mycobacterium avium and Mycobacterium tuberculosis by a mycobacteriophage delivered by a nonvirulent mycobacterium: a model for phage therapy of intracellular bacterial pathogens. J. Infect. Dis. 186, 1155-1160 (2002).
Intracellular bacterial infections are often difficult to treat and this paper provides evidence that phage could provide a therapeutic approach to this problem.
26. Smith, H. W. & Huggins, M. B. Successful treatment of experimental E. coli infections in mice using phage: its general superiority over antibiotics. J. Gen. Microbiol. 128, 307-318 (1982).
This is a crucial study in which fewer resistant bacterial colonies were found following phage therapy than found following antibiotic therapies, and the phage-resistant bacterial colonies were reported to have alterations in their capsules associated with reduced pathogenic properties.
27. Smith, H. W., Huggins, M. B. & Shaw, K. M. The control of experimental E. coli diarrhea in calves by means of bacteriophages. J. Gen. Microbiol. 133, 1111-1126 (1987).
28. Smith, H. W., Huggins, M. B. & Shaw, K. M. Factors influencing the survival and multiplication of bacteriophages in calves and their environments. J. Gen. Microbiol. 133, 1127-1135 (1987).
29. Ramesh, V., Fralick, J. A. & Rolfe, R. D. Prevention of Clostridium difficile -induced ileocecitis with bacteriophage. Anaerobe 5, 69-78 (1999).
30. Soothill, J. S. Bacteriophage prevents destruction of skin grafts by Pseudomonas aeruginosa . Burns 20, 209-211 (1994).
31. Nakai, T. & Park, S. C. Bacteriophage therapy for infectious diseases in aquiculture. Res. Microbiol. 153, 13-18 (2002).
32. Flaherty, J. E., Harbaugh, B. K., Jones, J. B., Somodi, G. C. & Jackson, L. E. H-mutant bacteriophages as a potential biocontrol of bacterial blight of geraniums. Hortscience 36, 90-100 (2001).
33. Flaherty, J. E., Jones J. B., Harbaugh, B. K., Somodi, G. C. & Jackson, L. E. Control of bacterial spot on tomato in the greenhouse and field with H-mutant bacteriophages. Hortscience 35, 882-884 (2000).
34. Geier, M. R., Trigg, M. E. & Merril, C. R. The fate of bacteriophage [lambda] in non-immune germ-free mice. Nature 246, 221-223 (1973).
This paper highlights the distribution of functional phage administered by various routes in mice and it presents evidence that oral administration is an ineffective method for achieving a systemic distribution of phage.
35. Appelmans, R. Le bacteriophage dans l’organisme. Comp. Rend. Soc. de Biol. (Paris) 85, 722-724 (1921).
36. Nungester, W. J. & Watrous, R. M. Accumulation of bacteriophage in spleen and liver following its intravenous inoculation. Proc. Soc. Exper. Biol. Med. 31, 901-905 (1934).
37. Inchley, C. J. The activity of mouse kupffer cells following intravenous injection of T4 bacteriophage. Clin. Exp. Immunol. 5, 173-187 (1969).
The crucial role of the liver in removing phage from the circulation of mammals is clearly delineated in this study.
38. Merril, C. R. et al . Long-circulating bacteriophage as antibacterial agents. Proc. Natl Acad. Sci. USA 93, 3188-3192 (1996).
This paper describes the development of a selection technique, based on the recognition that the efficacy of phage therapy might be impaired by the mammalian innate immune system, for obtaining long-circulating phage with enhanced therapeutic properties.
39. Doerfler, W. et al . On the insertion of foreign DNA into mammalian genomes: mechanism and consequences. Gene 157, 241-245 (1995).
40. Schubbert, R., Hohlweg, U., Renz, D. & Doerfler, W. On the fate of orally ingested foreign DNA in mice: chromosomal association and placental transmission to the fetus. Mol. Gen. Genet. 259, 569-576 (1998).
41. Schubbert, R., Renz, D., Schmitz, B. & Doerfler, W. Foreign (M13) DNA ingested by mice reaches peripheral leukocytes, spleen, and liver via the intestinal wall mucosa and can be covalently linked to mouse DNA. Proc. Natl Acad. Sci. USA 94, 961-966 (1997).
42. Merril, C. R., Geier, M. R. & Petricciani, J. C. Bacterial virus gene expression in human cells. Nature 233, 398-400 (1971).
43. Horst, J., Kluge, F., Beyreuther, K. & Gerok, W. Gene transfer to human cells: transducing phage [lambda] plac gene expression in GM1-gangliosidosis fibroblasts. Proc. Natl Acad. Sci. USA 72, 3531-3535 (1975).
44. Larocca, D. et al . Evolving phage vectors for cell targeted gene delivery. Curr. Pharm. Biotechnol. 3, 45-57 (2002).
45. Kucharewica-Krukowska A. & Slopek S. Immunogenic effect of bacteriophage in patients subjected to phage therapy. Arch Immunol. Ther. Exp. (Warsz.) 35, 553-561 (1987).
46. Levin, B. R. & Bull, J. J. Phage therapy revisited: the population biology of a bacterial infection and its treatment with bacteriophage and antibiotics. Am. Nat. 147, 881-898 (1996).
47. Payne, R. J. H. & Jansen, V. A. A. Pharmacokinetic principles of bacteriophage therapy. Clin. Pharmacokinet. 42, 315-325 (2003).
48. Francis, K. P. et al . Visualizing Pneumococcal infections in the lungs of live mice using bioluminescent Streptococcus pneumoniae transformed with a novel Gram-positive lux transposon. Infect. Immun. 69, 3350-3358 (2001).
Visualization methods presented in this study could facilitate the study of bacterial infections and their treatment.
49. Ochs, H. D., Davis, S. D. & Wedgwood, R. J. Immunologic responses to bacteriophage [phi]X174 in immunodeficiency diseases. J. Clin. Invest. 50, 2559-2568 (1971).
This paper presents some of the initial experiments using phage to probe the human and mammalian immune systems.
50. Ochs, H. D., Nonoyama, S., Zhu, Q., Farrington, M. & Wedgwood, R. J. Regulation of antibody responses: the role of complement and adhesion molecules. Clin. Immunol. Immunopathol. 3, S33-S40 (1993).
51. Clark, L., Greenbaum, C., Jiang, J., Lernmark, Å. & Ochs, H. The antibody response to bacteriophage is linked to the lymphopenia gene in congenic BioBreeding rats. FEMS Immunol. Med. Microbiol. 32, 205-209 (2002).
52. Ching, Y -C., Davis, S. D. & Wedgwood, R. J. Antibody studies in hypogammaglobulinemia. J. Clin. Invest. 45, 1593-1600 (1966).
53. Jenne, S., Brepoels, K., Collen, D. & Jespers, L. High-resolution mapping of the B cell epitopes of staphylokinase in humans using negative selection of a phage-displayed antigen library. J. Immunol. 161, 3161-3168 (1998).
54. Bartlett, J. G. Antibiotic-associated diarrhea. N. Engl. J. Med. 346, 334-339 (2002).
55. Scholl, D., Rogers, S., Adhya, S. & Merril, C. Bacteriophage K1-5 encodes two different tail fiber proteins allowing it to infect and replicate on both K1 and K5 strains of E. coli . J. Virol. 75, 2509-2515 (2001).
Adaptations of the phage construct presented in this paper could provide a general approach for the extension of the bacterial host range of phage.
56. Scholl, D., Adhya, S. & Merril, C. R. Bacteriophage SP6 is closely related to phages K1-5, K5 and K1E but encodes a tail protein very similar to that of the distantly related P22. J. Bacteriol. 184, 2833-2836 (2002).
57. Sandmeier, H. Acquisition and rearrangement of sequence motifs in the evolution of bacteriophage tail fibres. Mol. Microbiol. 12, 343-350 (1994).
58. Liu, M. et al . Reverse transcriptase-mediated tropism switching in bordetella bacteriophage. Science 295, 2091-2094 (2002).
59. Moffatt, B. A. & Studier, F. W. Entry of bacteriophage T7 DNA into the cell and escape from host restriction. J. Bacteriol. 170, 2095-2105 (1988).
60. Hollon, T. Impossible vaccine tames Staphylococcus aureus . The Scientist 16, 24-28 (2002).
61. Gabig, M. et al . The cell surface protein Ag43 facilitates phage infection of Escherichia coli in the presence of bile salts and carbohydrates. Microbiology 148, 1533-1542 (2002).
62. Danese, P. N., Pratt, L. A., Dove, S. L. & Kolter, R. The outer membrane protein, antigen 43, mediates cell-to-cell interactions within Escherichia coli biofilms. Mol. Microbiol. 37, 424-432 (2000).
63. Colvin, M. G. Behavior of bacteriophage in body fluids and in exudates. J. Infect. Dis. 51, 527-541 (1932).
64. Calalb, G. Action de la bile sur bacteriophage et importance de cette action. Compt. Rend. Soc. De biol. (Paris) 92, 1442-1443 (1925).
65. Wagner, P. L. & Waldor, M. K. Bacteriophage control of bacterial virulence. Infect. Immun. 70, 3985-3993 (2002).
66. Altschul, S. F., Gish, W., Miller, W., Myers, E. W. & Lipman, D. J. Basic local alignment search tool. J. Mol. Biol. 215, 403-410 (1990).
67. Loessner, M. J., Rees, C. E. D., Steward, A. B. & Scherer, S. Construction of luciferase reporter bacteriophage A511::luxAB for rapid and sensitive detection of viable Listeria cells. Appl. Environ. Microbiol. 62, 1133-1140 (1996).
68. Carriere, C. J. et al . Conditionally replicating luciferase reporter phages: improved sensitivity for rapid detection and assessment of drug susceptibility of Mycobacterium tuberculosis . J. Clin. Microbiol. 35, 3232-3239 (1997).
69. Schuch, R., Nelson, D. & Fischetti, V. A. A bacteriolytic agent that detects and kills Bacillus anthracis . Nature 418, 884-889 (2002).
70. Lay, J. O. Jr MALDI-TOF mass spectrometry of bacteria. Mass Spectrom. Rev. 20, 172-194 (2001).
71. Van Baar, B. L. M. Characterization of bacteria by matrix-assisted laser desorption/ionisation and electrospray mass spectrometry. FEMS Microbiol. Rev. 24, 193-219 (2000).
72. Hamels, S. et al . Consensus PCR and microarray for diagnosis of the genus Staphylococcus species and methicillin resistance. BioTechniques 31, 1364-1366, 1368, 1370-1372 (2001).
73. Uhr, J. W., Finkelstein, M. S. & Baumann, J. B. Antibody formation: III. the primary and secondary antibody response to bacteriophage [psi]X 174 in guinea pigs. J. Exp. Med. 115, 655-670 (1962).
74. Lederberg, J. Smaller fleas...ad infinitum: therapeutic bacteriophage redux. Proc. Natl Acad. Sci. USA 93, 3167-3168 (1996).
This review stresses the need for additional research to facilitate the use of these viruses as safe and effective therapeutic antibacterial agents.
75. Knight, J. Superbugs reveal chink in armour. Nature 417, 477 (2002).
76. Kilman, S. FDA restricts antibiotic use in livestock to protect people. The Wall Street Journal D3 (12 September, 2002).
77. Merril, C. R. et al . Isolation of bacteriophages from commercial sera. In Vitro 8, 91-93 (1972).
78. Merril, C. R. Phage in human vaccines. Science 188, 8 (1975).
79. Bernhardt, T. G., Wang, I -N., Struck, D. K. & Young, R. A protein antibiotic in the phage Qb virion: diversity in lysis targets. Science 292, 2326-2329 (2001).
80. Nelson, D., Loomis, L. & Fischetti, V. A. Prevention and elimination of upper respiratory colonization of mice by group A streptococci by using a bacteriophage lytic enzyme. Proc. Natl Acad. Sci. USA 98, 4107-4112 (2001).
81. Gaeng, S., Scherer, S., Neve, H. & Loessner, M. J. Gene cloning and expression and secretion of Listeria monocytogenes bacteriophage-lytic enzymes in Lactococcus lactis . Appl. Environ. Microbiol. 66, 2951-2958 (2000).
82. Naidu, B. P. B. & Avari, C. R. Bacteriophage in the treatment of plague. Ind. J. Med. Res. 19, 737-748 (1932).
83. Boyd, E. F., Davis, B. M. & Hochhut, B. Bacteriophage-bacteriophage interactions in the evolution of pathogenic bacteria. Trends Microbiol. 9, 137-144 (2001).
Author Affiliation(s):
[1] Section on Biochemical Genetics, National Institute of Mental Health, National Institutes of Health, Bethesda, Maryland 20892, USA.
Email: merrilc@helix.nih.gov
Email: dscholl@helix.nih.gov
[2] Section of Developmental Genetics, National Cancer Institute, National Institutes of Health, Bethesda, Maryland 20892, USA.
Email: sadhya@helix.nih.gov
Author Bio(s):
Carl R. Merril is the chief of the Section on Biochemical Genetics at the National Institute of Mental Health (NIHM), National Institutes of Health (NIH). He has co-authored 225 articles, and 23 patents. His research ranges from basic and applied bacteriophage studies to the development of sensitive protein detection methods, including the silver stains. One of his publications concerning this methodology was declared a citation classic by the journal Current Contents as it earned more than 2,500 citations since its publication. In addition, two of his patents in this field have earned recognition as top money-makers for the Public Health Service (PHS), defined as a PHS-invented commercialized product that exceeds US $100,000 in annual sales. He has received a number of awards including the PHS Distinguished Service Medal and the Surgeon General’s Exemplary Service Medal.
Dean Scholl is a fellow in the Section on Biochemical Genetics at the NIMH, NIH. He has co-authored eight papers and three patents.
Sankar L. Adhya is the chief of the Section on Developmental Genetics, National Cancer Institute, NIH. He has co-authored more than 150 articles and 10 patents. He has received a number of awards, including election to the US National Academy of Sciences, the Indian Academy of Sciences and the American Academy of Microbiology.
DOI: 10.1038/nrd1111
.................................................................
Sea Sponge Extract Conquers Resistant Bacteria
Science News – 14 Mar 09
Science News has an article on research into a compound
found in a particular kind of sea sponge that seems to have the ability to restore
antibiotics' effectiveness against resistant bacteria. The hope is that,
since the compound is not itself deadly or even harmful to bacteria, it may
skew the antibiotic-bacteria arms race in our favor. "Chemical analyses
of the sponge's chemical defense factory pointed to a compound called
algeferin. Biofilms, communities of bacteria notoriously resistant to
antibiotics, dissolved when treated with fragments of the algeferin molecule.
And new biofilms did not form. So far, the algeferin offshoot has, in the lab,
successfully treated bacteria that cause whooping cough, ear infections,
septicemia and food poisoning. The compound also works on... [MRSA] infections,
which wreak havoc in hospitals. 'We have yet to find one that doesn't work,'
says [one of the researchers]."
Sponge’s secret weapon restores antibiotics’ power
Bacteria treated with compound lose their resistance
CHICAGO — A
chemical from an ocean-dwelling sponge can reprogram antibiotic resistant
bacteria to make them vulnerable to medicines again, new evidence suggests.
Ineffective antibiotics become lethal once again for bacteria treated with the sponge compound, chemist Peter Moeller reported February 13 at the American Association for the Advancement of Science annual meeting.
“The potential is outstanding. This could revolutionize our approach to thinking about how infections are treated,” comments Carolyn Sotka of the National Oceanic and Atmospheric Administration’s Oceans and Human Health Initiative in Charleston, S.C.
Everything living in the ocean survives in a microbial soup, under constant bombardment from bacterial assaults. Researchers led by Moeller, of Hollings Marine Laboratory in Charleston, found a sponge thriving in the midst of dead organisms. This anomalous life amidst death raised an obvious question, says Moeller: “How is this thing surviving when everything else is dead?”
Chemical analyses of the sponge’s chemical defense factory pointed to a compound called ageliferin. Biofilms, communities of bacteria notoriously resistant to antibiotics, dissolved when treated with fragments of the ageliferin molecule. And new biofilms did not form.
So far, the ageliferin offshoot has, in the lab, successfully resensitized bacteria that cause whooping cough, ear infections, septicemia and food poisoning. The compound also works on Pseudomonas aeruginosa, which causes horrible infections in wounded soldiers, and MRSA infections, which wreak havoc in hospitals. “We have yet to find one that doesn’t work,” says Moeller.
And the results may not just apply to bacteria in communities. The compound is able to reprogram antibiotic-resistant bacteria that don’t form biofilms. When bacteria are treated with the compound, antibiotics that usually have no effect are once again lethal. This substance may be the first one that can eliminate bacteria's resistance, Moeller says. “This resensitization is brand new.”
And the problem of perpetuating a bacterial-resistance arms race, in which bacteria rapidly develop countermeasures against new antibiotics, may be avoided entirely with the new compound. “Since the substance is nontoxic to the bacterium, it’s not throwing up any red flags,” says Moeller.
Other than “doing something really funky that we’re excited about,” researchers don’t yet know how this compound interferes with bacterial resistance to antibiotics, says Moeller. The compound may sneak by bacteria’s sensors that trigger new ways to combat antibiotics. Bacteria continually treated with this compound for three months are still susceptible to antibiotics.
The research is still in very early phases.
“Everyone would like to see this in antibiotic trials tomorrow,” Moeller says, but treatments for human infections are a long way off.
Sotka agrees. “Of course, we need clinical trials to take it to the next level,” she says.
Ineffective antibiotics become lethal once again for bacteria treated with the sponge compound, chemist Peter Moeller reported February 13 at the American Association for the Advancement of Science annual meeting.
“The potential is outstanding. This could revolutionize our approach to thinking about how infections are treated,” comments Carolyn Sotka of the National Oceanic and Atmospheric Administration’s Oceans and Human Health Initiative in Charleston, S.C.
Everything living in the ocean survives in a microbial soup, under constant bombardment from bacterial assaults. Researchers led by Moeller, of Hollings Marine Laboratory in Charleston, found a sponge thriving in the midst of dead organisms. This anomalous life amidst death raised an obvious question, says Moeller: “How is this thing surviving when everything else is dead?”
Chemical analyses of the sponge’s chemical defense factory pointed to a compound called ageliferin. Biofilms, communities of bacteria notoriously resistant to antibiotics, dissolved when treated with fragments of the ageliferin molecule. And new biofilms did not form.
So far, the ageliferin offshoot has, in the lab, successfully resensitized bacteria that cause whooping cough, ear infections, septicemia and food poisoning. The compound also works on Pseudomonas aeruginosa, which causes horrible infections in wounded soldiers, and MRSA infections, which wreak havoc in hospitals. “We have yet to find one that doesn’t work,” says Moeller.
And the results may not just apply to bacteria in communities. The compound is able to reprogram antibiotic-resistant bacteria that don’t form biofilms. When bacteria are treated with the compound, antibiotics that usually have no effect are once again lethal. This substance may be the first one that can eliminate bacteria's resistance, Moeller says. “This resensitization is brand new.”
And the problem of perpetuating a bacterial-resistance arms race, in which bacteria rapidly develop countermeasures against new antibiotics, may be avoided entirely with the new compound. “Since the substance is nontoxic to the bacterium, it’s not throwing up any red flags,” says Moeller.
Other than “doing something really funky that we’re excited about,” researchers don’t yet know how this compound interferes with bacterial resistance to antibiotics, says Moeller. The compound may sneak by bacteria’s sensors that trigger new ways to combat antibiotics. Bacteria continually treated with this compound for three months are still susceptible to antibiotics.
The research is still in very early phases.
“Everyone would like to see this in antibiotic trials tomorrow,” Moeller says, but treatments for human infections are a long way off.
Sotka agrees. “Of course, we need clinical trials to take it to the next level,” she says.
...............................................
While the government invokes the spirit of Florence Nightingale in a -
surely desperate - bid to tackle the growing problem of antibiotic resistance
in hospitals, at least two UK biotech firms are engaged in a race to come up
with a 21st century solution. Both companies are also using a rather elderly
technique - discovered during the First World War - but bringing it up to date
with modern genetics.
While the government invokes the spirit of Florence Nightingale in a - surely desperate - bid to tackle the growing problem of antibiotic resistance in hospitals, at least two UK biotech firms are engaged in a race to come up with a 21st century solution. Both companies are also using a rather elderly technique - discovered during the First World War - but bringing it up to date with modern genetics.
The winner will be the first to market an antibacterial product containing a type of virus know as a "bacteriophage" - literally "bacteria eater". First discovered in 1917 by the Frenchman Felix d'Herelle, "phages" were used to treat conditions like infected wounds, ulcers, typhoid and cholera for about 20 years but then, on the advent of antibiotics, were forgotten in the West
.
But phages are generating huge interest in research labs because, being alive, they are able to mutate, making it much harder for bacteria to develop resistance to them. A recent study in Science found that the phage that attacks Bordetella, which causes whooping cough, can make billions of variations in a key protein. Such versatility makes resistance unlikely.
Something new is certainly needed. A few years ago the first original antibiotic compound for 35 years was introduced. Within two months resistance to it had developed.
At least two of the companies in the race are working on phages to target MRSA (methicillin-resistant Staphylococcus aureus) the main bacterium involved in hospital-acquired infections that kill at least 5,000 people a year.
Each phage only infects a specific strain of bacteria, avoiding the carpet-bombing approach of antibiotics, which knock out friendly gut bacteria as well. Phages are also everywhere - probably the most numerous life form on the planet; a millilitre of water from a river will contain about 200 million of them. "We've patented a way of collecting phages from the wild," says Nick Housby of Novolytics, one of the companies in this race. "If a new, resistant strain of MRSA emerged in hospitals we could have a phage to attack it within a matter of weeks," he adds.
At least they could in maybe three or four years time, when their cocktail of about eight different phages, one for each of the main resistant strains of MRSA, has passed all the trials. Their first product will be a nasal spray to kill off the MRSA that 30 per cent of people carry harmlessly in their respiratory system, but which can be deadly to people with weakened immune systems in hospital.
Although still fairly novel in the West, phages have long been used in Russia. Phage-impregnated bandages were widely used by Soviet troops. One refugee from the main bacteriophage research and production lab in Georgia is now heading an American company called Intralytix. Recently the company obtained the first licence for the commercial use of phages on animals to combat listeria, which contaminates food and can seriously affect pregnant women, newborns, and adults with weakened immune systems.
Phage-based treatments are still sold over the counter in some eastern-European countries, their use supported by years of clinical experience, although little of it backed by conventional trials. The only detailed account of their use was published by the Polish Academy of Sciences, which summarised the effectiveness of phage therapy on 550 patients in 10 hospitals who were suffering from serious conditions such as septicaemia, abscesses, broncho-pneumonia and fistulas. The reported recovery rate was 94 per cent.
Such reports cut little ice with the UK regulatory authorities, so the race is on to do the first clinical trial with humans using phages, not just in the UK but anywhere in the West. Those at a firm called Biocontrol believe they are the front runners. "Some time in the next few months we will be placing a phage solution in the ears of patients who have become infected following surgery," says the chief scientific officer of the company, Dr David Harper.
The bug they are targeting is called Pseudomonas aeruginosa which is responsible for, among other things, chronic ear infections and the clogging mucus found in the lungs of people with cystic fibrosis. "We've already run a successful trial on 10 dogs who had failed several rounds of antibiotic treatment," says Harper.
But perhaps the most ingenious new phage line is coming from a firm called Phico Therapeutics. "While I was working in the States some years ago I discovered this protein that is able to totally shut down a bacterium's DNA," says Heather Fairhead, the founder of the company. "The protein is only found in a species of bacterium that forms spores when food supplies run low," she explains. "It goes into a kind of suspended animation and all its DNA becomes inactive." In Fairhead's system the phage is only used as a delivery vehicle - "its one aim in life is to target bacterial DNA, so it's perfect". The first application will be a barrier cream for potential MRSA carriers in hospitals.
Sales of a successful product could be huge, and the rivalry between the contenders is hotting up. "I should point out that we aren't using any genetic modification in our product," Housby of Novolytics e-mailed me "and our phages keep on reproducing, which Phico's don't. Fairhead was equally keen to stress her rivals' shortcomings. "When you kill bacteria using wild phages," she explained "they make the bacteria burst, so toxins get spewed out, along with genetic material that can carry resistance."
It's to sort out such possible issues that the trials need to be done. For instance, although there should be no problems putting phages into creams or ointments, some experts worry about putting them directly into the body. "There's the possibility of the phage being mopped up by the immune system or causing an allergic response," warns Geoffrey Hanlon of Brighton University.
There is a nice symmetry about the notion that an alliance between the principles of Florence Nightingale and a revamped bit of Russian health care may eventually roll back the advancing bacterial hordes.
..............................
http://www.sciencefriday.com
In the days before modern antibiotics, some researchers saw bacteriophages,
viruses that can seek out and destroy bacteria, as a promising candidate for
fighting infections. Now, as more organisms develop resistance to existing
antibiotics, phage research is finding new favor.
At the Society for General Microbiology meeting in Edinburgh, researchers presented work on incorporating bacteriophages into dressings for wounds and cleaning materials used in hospitals. The scientists found a way to bind the phages to polymer particles, allowing the viruses to remain active for up to three weeks rather than breaking down after a few hours. The hope is that the phage-based approach will provide new weapons in the battle against dangerous bacteria such as Methicillin-resistant Staphylococcus aureus (MRSA). In this segment, Ira and guests talk about bacteriophages and their place in modern medicine. Teachers, find more information about using Science Friday as a classroom resource in the Kids' Connection.
Vice-President, Research and Development
Chief Scientist Intralytix, Inc. Baltimore, Maryland
Thomas Hausler Author: "Viruses vs. Superbugs: A Solution to the Antibiotics Crisis," (Macmillan, 2007)
Science Reporter, Swiss Public Radio Basel, Switzerland
 Bacteriophage Simulated Image
Bacteriophage Simulated Image
.................................
The new antibiotics
“The Independent” – Health and Wellbeing
They can fight infections, promise fewer side effects and can
adapt when diseases resist them. Bacteriophages could be the answer to the MRSA
superbug. Jerome Burne reports
Tuesday, 16
November 2004
While the government invokes the spirit of Florence Nightingale in a - surely desperate - bid to tackle the growing problem of antibiotic resistance in hospitals, at least two UK biotech firms are engaged in a race to come up with a 21st century solution. Both companies are also using a rather elderly technique - discovered during the First World War - but bringing it up to date with modern genetics.
The winner will be the first to market an antibacterial product containing a type of virus know as a "bacteriophage" - literally "bacteria eater". First discovered in 1917 by the Frenchman Felix d'Herelle, "phages" were used to treat conditions like infected wounds, ulcers, typhoid and cholera for about 20 years but then, on the advent of antibiotics, were forgotten in the West
.
But phages are generating huge interest in research labs because, being alive, they are able to mutate, making it much harder for bacteria to develop resistance to them. A recent study in Science found that the phage that attacks Bordetella, which causes whooping cough, can make billions of variations in a key protein. Such versatility makes resistance unlikely.
Something new is certainly needed. A few years ago the first original antibiotic compound for 35 years was introduced. Within two months resistance to it had developed.
At least two of the companies in the race are working on phages to target MRSA (methicillin-resistant Staphylococcus aureus) the main bacterium involved in hospital-acquired infections that kill at least 5,000 people a year.
Each phage only infects a specific strain of bacteria, avoiding the carpet-bombing approach of antibiotics, which knock out friendly gut bacteria as well. Phages are also everywhere - probably the most numerous life form on the planet; a millilitre of water from a river will contain about 200 million of them. "We've patented a way of collecting phages from the wild," says Nick Housby of Novolytics, one of the companies in this race. "If a new, resistant strain of MRSA emerged in hospitals we could have a phage to attack it within a matter of weeks," he adds.
At least they could in maybe three or four years time, when their cocktail of about eight different phages, one for each of the main resistant strains of MRSA, has passed all the trials. Their first product will be a nasal spray to kill off the MRSA that 30 per cent of people carry harmlessly in their respiratory system, but which can be deadly to people with weakened immune systems in hospital.
Although still fairly novel in the West, phages have long been used in Russia. Phage-impregnated bandages were widely used by Soviet troops. One refugee from the main bacteriophage research and production lab in Georgia is now heading an American company called Intralytix. Recently the company obtained the first licence for the commercial use of phages on animals to combat listeria, which contaminates food and can seriously affect pregnant women, newborns, and adults with weakened immune systems.
Phage-based treatments are still sold over the counter in some eastern-European countries, their use supported by years of clinical experience, although little of it backed by conventional trials. The only detailed account of their use was published by the Polish Academy of Sciences, which summarised the effectiveness of phage therapy on 550 patients in 10 hospitals who were suffering from serious conditions such as septicaemia, abscesses, broncho-pneumonia and fistulas. The reported recovery rate was 94 per cent.
Such reports cut little ice with the UK regulatory authorities, so the race is on to do the first clinical trial with humans using phages, not just in the UK but anywhere in the West. Those at a firm called Biocontrol believe they are the front runners. "Some time in the next few months we will be placing a phage solution in the ears of patients who have become infected following surgery," says the chief scientific officer of the company, Dr David Harper.
The bug they are targeting is called Pseudomonas aeruginosa which is responsible for, among other things, chronic ear infections and the clogging mucus found in the lungs of people with cystic fibrosis. "We've already run a successful trial on 10 dogs who had failed several rounds of antibiotic treatment," says Harper.
But perhaps the most ingenious new phage line is coming from a firm called Phico Therapeutics. "While I was working in the States some years ago I discovered this protein that is able to totally shut down a bacterium's DNA," says Heather Fairhead, the founder of the company. "The protein is only found in a species of bacterium that forms spores when food supplies run low," she explains. "It goes into a kind of suspended animation and all its DNA becomes inactive." In Fairhead's system the phage is only used as a delivery vehicle - "its one aim in life is to target bacterial DNA, so it's perfect". The first application will be a barrier cream for potential MRSA carriers in hospitals.
Sales of a successful product could be huge, and the rivalry between the contenders is hotting up. "I should point out that we aren't using any genetic modification in our product," Housby of Novolytics e-mailed me "and our phages keep on reproducing, which Phico's don't. Fairhead was equally keen to stress her rivals' shortcomings. "When you kill bacteria using wild phages," she explained "they make the bacteria burst, so toxins get spewed out, along with genetic material that can carry resistance."
It's to sort out such possible issues that the trials need to be done. For instance, although there should be no problems putting phages into creams or ointments, some experts worry about putting them directly into the body. "There's the possibility of the phage being mopped up by the immune system or causing an allergic response," warns Geoffrey Hanlon of Brighton University.
There is a nice symmetry about the notion that an alliance between the principles of Florence Nightingale and a revamped bit of Russian health care may eventually roll back the advancing bacterial hordes.
..............................
THIS PAGE IS DESIGNED TO BRING MP3 FILES
TO YOUR ATTENTION.
"Science Friday" has some excellent podcasts available and some are situated below, where they are relevant to issues raised in this Website.http://www.sciencefriday.com
Phages Fight Bacteria (broadcast Friday, April 4th, 2008)
(The image below depicts the structure of the T4 virus, one type
of bacteriophage. Frederick A. Eiserling/UCLA and Petr Leiman/Purdue Department
of Biological)
At the Society for General Microbiology meeting in Edinburgh, researchers presented work on incorporating bacteriophages into dressings for wounds and cleaning materials used in hospitals. The scientists found a way to bind the phages to polymer particles, allowing the viruses to remain active for up to three weeks rather than breaking down after a few hours. The hope is that the phage-based approach will provide new weapons in the battle against dangerous bacteria such as Methicillin-resistant Staphylococcus aureus (MRSA). In this segment, Ira and guests talk about bacteriophages and their place in modern medicine. Teachers, find more information about using Science Friday as a classroom resource in the Kids' Connection.
Guests
Alexander SulakvelidzeVice-President, Research and Development
Chief Scientist Intralytix, Inc. Baltimore, Maryland
Thomas Hausler Author: "Viruses vs. Superbugs: A Solution to the Antibiotics Crisis," (Macmillan, 2007)
Science Reporter, Swiss Public Radio Basel, Switzerland
Related Links
- Antibacterial Phage Therapy
- The Bacteriophage Ecology Group
- Wired: How Ravenous Soviet Viruses Will Save the World
- Thomas Hausler: 'Viruses vs Superbugs'

.................................
Division
M is composed of researchers and teachers dedicated to the study of
bacterial viruses. Current topics of interest are: assembly and
structure, genome structure, initiation of infection, regulation of
transcription and translation, replication, recombination, repair,
virus-host interactions, new phage systems, molecular cloning
technology, applications of phage & phage products, and
bacteriophage evolution.
Words in this text marked are linked to glossary entries.
What is a bacteriophage, anyway?
A brief introduction to the beast, complete with pronunciation guide.
Members
of Division M certainly know what bacteriophages are, but other readers
of this page may wonder what it is about these tiny microorganisms that
would make so many scientists devote their professional lives to
understanding how they work. This part of the site provides a brief
primer for the uninitiated about what bacteriophages are, what they do,
and what they do for us; and gives a quick refresher for those who once
knew something about bacteriophages. Teachers who wish to include
bacteriophages in their curricula will find some useful links in our
"Resources for teachers", "Books", and "Links" pages.
- What is a bacteriophage—the basics
- Abundance & variety of bacteriophages
- History of bacteriophage research
- The practical phage— Human uses of bacteriophages
Bacteriophages
(“phages” for short) are viruses whose hosts are bacterial cells. Like
all viruses, phages are metabolically inert in their extracellular form
(the “virion”), and they reproduce by insinuating themselves into the
metabolism of the host. The mechanisms by which phage virions infect
their host cells—described in more detail below—vary among the different
types of phages, but they all result in delivery of the phage genome
into the cytoplasm of the bacterial host, where it interacts with the
cellular machinery to carry the phage life cycle forward. The result of
infection can be, and often is, total devastation for the cell. A good
example of this is infection by the E. coli phage T4, the Tyrannosaurus rex
of phages, which commandeers the material and energetic resources of
the cell and turns them toward making more virions, after which it
causes violent lysis of the cell and release of the progeny virions. At
another extreme, the large group of phages known as temperate phages have the option when they infect of setting up a state of coexistence with the host ( “lysogeny”)
in which the genes that would harm the host are prevented from being
expressed, while a small set of genes that provide benefit to the host
are expressed. Both scenarios result in replication and perpetuation of
the bacteriophage.
Follow this link for guidance on pronouncing the words ‘bacteriophage’ and ‘phage’.
There
are probably more individual bacteriophages in the biosphere than there
are of any other group of organisms, including all the prokaryotes.
Until recently nobody knew how to get even an approximate estimate of
how many phages there are, but a little over ten years ago, it occurred
to someone that at least for the best studied group of phages, the
tailed phages, their shape is so distinctive that their numbers in
aquatic environments could be estimated simply by centrifuging them onto
an electron microscope sample grid and counting them. Astonishingly, in
coastal sea water there are typically as many as 10 7 (ten million) tailed phages per milliliter. In some fresh water sources there are up to 10 9
(a billion) per milliliter. Although there is still little information
about how uniform is the distribution of phages around the globe, these
numbers give at least a rough basis for calculating the global
population. The remarkable result of such a calculation is that there
may be as many as 10 30
tailed phage globally. For people who like their numbers written out,
that’s 1,000,000,000,000,000,000,000,000,000,000. If you were to gather
them all up and weigh them, they would outweigh the world population of
elephants by a thousand-fold or more.
The
tailed phages are also known as the dsDNA tailed phages because their
genomes are molecules of linear double-stranded DNA. Their genomes are
relatively large for viruses, with most of them in the vicinity of 50
kbp (50,000 base pairs). However, some are less than 20 kbp, the common
and well studied ‘T4-like’ group is more like 160 kbp, and bacteriophage
G is the largest virus on record, with a genome of nearly 500
kbp—bigger than the smallest bacterial genomes.
Although
the dsDNA tailed phages account for about 95% of all phages reported in
the scientific literature, and may in fact make up the majority of
phages on the planet, there are other phages that occur abundantly in
the Biosphere sporting very different virions, genomes, and lifestyles.
These are listed in more detail in the "Phage Facts & Portraits"
pages on this site, but they include phages with ssDNA, ssRNA, or
segmented dsRNA genomes, virions with and those without membrane
components, and many other differences. In fact, the diversity of phages
is at least as great as the diversity of plant and animal viruses, in
keeping with the probability that phages and viruses of eukaryotes share common ancestry.
Bacteriophages
were discovered a little over 80 years ago—in 1915 by the Englishman
Frederick Twort and independently in 1917 by the French Canadian Félix
D’Herelle. Initial research on phage was concerned with defining the
nature of the bacteriophage—the two leading theories being that it was a
filterable virus, like the Tobacco Mosaic Virus that had been
discovered some 20 years earlier, or a self-perpetuating enzyme whose
expression caused destruction of the bacterial cell.
Regardless
of the exact nature of the bacteriophage, it was quickly realized that
bacteriophages had the potential to kill the bacteria that cause many
infectious diseases in humans, as well as in agriculturally important
plants and animals. This idea formed the basis for much research as well
as for the Pulitzer Prize-winning 1924 novel Arrowsmith by Sinclair
Lewis (still a good read).
Félix D’Herelle in particular was a champion of the potential for
therapeutic uses of phage, which he promoted vigorously. In 1933,
D’Herelle co-founded an institute for phage research in the Soviet
Republic of Georgia, together with Georgian microbiologist George
Eliava. Although Eliava was killed in one of Stalin’s purges in 1937,
and D’Herelle never returned, the G. Eliava Institute of Bacteriophage survived and continued to supply phage for therapeutic uses to the entire Soviet Union until the recent breakup of the Soviet Union.
In the West, research on such ‘phage therapy’ was dropped when
penicillin and other chemical antibiotics were discovered starting in
the 1940’s, though there has been some renewed interest in phage therapy in recent years as antibiotic resistance of pathogenic bacteria has become a more prominent threat to public health.
Meanwhile,
bacteriophage research continued. The viral nature of the bacteriophage
was clearly established, the chemical composition of the virions (the
extracellular virus particles) was measured and shown to be protein and
DNA, new phages infecting a variety of bacterial hosts were isolated,
and some rudimentary progress was made in understanding the virus life
cycle. The first electron micrographs of phages, showing a tadpole-like
shape, were obtained in 1942 by Tom Anderson.
The
‘modern’ era of bacteriophage research is usually dated from 1938 when
the expatriate German physicist, Max Delbrück, began his work on phages
at the California Institute of Technology. Salvadore Luria, an Italian
expatriate at Indiana University (later at MIT) and Al Hershey, an
American at Vanderbilt University (later at Cold Spring Harbor) soon
joined Delbrück in pursuing bacteriophage research as a route to
understanding the most fundamental features of biological life.
Phages
soon became central players in the foundation of the discipline that
later came to be known as molecular biology (the Journal of Molecular
Biology started publication in 1959). Through the 1950’s and 1960’s,
phage research had a dominant role
in elucidating the most fundamental facts about what genes are and how
the information in genes is read out to determine the properties of an
organism. An underlying assumption (and justification) of the early
phage molecular biologists was that the principles of life that could be
learned from phages would also apply to other forms of life. As it has
become clear in subsequent decades just how remarkably correct that
assumption was, it has become similarly clear that the history of phage
biology is a major and essential part of the modern history of biology
as a whole.
The
astonishing success of bacteriophage research over the 25-30 years
prior to about 1970 in revealing the fundamental ‘secrets of life’ can
be attributed largely to the fact that phages are so tractable as
experimental systems. That is, they are genetically and structurally
simple, they have a short life cycle
that can be synchronized in a population, and genetic, biochemical, and
structural approaches can be applied synergistically. The fact that
phages interact intimately with their bacterial hosts means that
virtually everything that is learned about phages is also informative
about the bacterial cells they infect, and often about even broader
biological questions.
Around 1970 the world of biological research began to be transformed by the ‘ recombinant DNA revolution’, with which it becomes possible to effectively change a gene from any organism—no matter how complex or how eukaryotic—into
a phage gene. The suite of laboratory techniques that made this
revolution possible was developed largely through research on phages
(with, of course, major contributions from research directed at their
bacterial hosts and their genetic cousins, the plasmids). The
recombinant DNA revolution has produced some profound changes in
bacteriophage research, as in all other areas of biological research.
For one thing, the number of researchers working primarily on phages
decreased precipitously as it became possible to study the genes of more
complex—particularly eukaryotic—organisms with nearly the same ease as
had been possible previously primarily with phages and bacteria. At the
same time, the number of biological researchers using some form of phage
in their research has increased substantially, since many of the tools
of modern molecular biological research are phages or phage-derived (see
The Practical Phage,
below). And just as recombinant DNA and other ‘modern’ techniques have
made it easier to study the molecular biology of fruit flies, elephants,
and sea slugs, they have also greatly increased the sophistication of
the experiments that can be done with phages. Thus for those scientific
problems where phages provide advantageous experimental systems,
bacteriophage research is still vigorous and in many cases leading the
field.
Because
phages attack bacteria, and bacteria are sometimes harmful to people,
many phage biologists believe it is possible to use phage or phage
products (such as phage-encoded enzymes) as disease therapy or in other
ways to solve our bacterial problems. At this writing, with a few
exceptions, these techniques are in research stages rather than in
actual use. Examples include treatment of particular bacterial
infections or infestations with specific phage, treatment of bacterial
infections with phage products, and use of phage-encoded toxins to
combat cancer. Among the issues that need resolution before application
of these methods becomes practical are how the phage-based therapeutic
agent is to be delivered to the patient, how to protect the phage-based
agent from immune attack by the patient's body, and how to handle the
expected development of phage-resistant pathogens.
On
the other hand, phages are and have for decades been widely used as
tools in recombinant DNA technology: important in applications and
developing applications ranging from medical diagnostics and forensics
to basic research. See above, History of bacteriophage research, and our page Major discoveries made with bacteriophages.
...........................................
A Glossary defining some terms for bacteriophage biology
Division M
[Division M is composed of researchers and teachers dedicated to the study of bacterial viruses]
Words in the text marked <G> indicate links to definitions elsewhere in this glossary.
Please see our note on web viewing of Greek letters in phage names.
To
view the illustrations (larger than the thumbnails) in this glossary
you must enable your browser for Java. Some of the images are animated.
A-B type toxins
are protein molecules secreted by bacteria, frequently as single
polypeptides that are later hydrolyzed to produce a B peptide, which
binds specifically to some target cell, linked to an A peptide, which
has some enzymatic activity harmful to cells. Details of subunit
secretion and composition of the mature toxin vary. It is the job of the
B peptide to get the A peptide into the cytoplasm of a particular type
of cell, where the A peptide performs its nasty activity to kill the
cell. The details of toxin internalization also vary, and not all are as
pictured in the illustrations here. It is the particular specificity of
the B peptide that determines what type of cell will be the target.
Some B peptides bind to nerve cells, others to gut cells, and so on. The
actual symptoms experienced by the person exposed to the toxin depend
on what type of cells are killed. Killing of nerve cells might cause
paralysis, and killing of gut cells might cause intestinal symptoms, for
example.
Illustrations for A-B type toxins (line drawings & animated GIF files:please enable your browser for Java)
1: 2: 3:
Antibiotic therapy
consists of treatment of an infected person, animal, or plant with a
chemical antimicrobial agent with the intent of controlling an
infection. The original definition of an antibiotic included the
requirement that the agent be one produced by another microorganism.
Although that is still often true, many synthetic derivatives of
antibiotics have been made, where modifications improve performance of
the agent, and these agents are usually also called antibiotics. The
microbe that is the target of the agent can be a fungus (antifungal
antibiotic) but is most often a bacterial pathogen (antibacterial
antibiotic). Although a few antiviral agents are in use, typically these
are not chemicals produced by microorganisms and so are not called
antibiotics. The conventional use of the term antibiotic implies that it
is antibacterial.
Therapeutically
successful antibiotics have a property called "selective toxicity".
These agents work by killing or interfering with the growth of some
parasite we don't want growing in us. But the fundamental chemistry of
how cells work is the same whether the cells are bacterial, fungal,
plant, bovine, or human. Chemical toxicity that would interfere with
chemistry we all have in common would also harm us, causing nasty or
even fatal "side effects". Most bacteria and fungi have cell walls that
are made of materials that don't occur in humans or our agricultural
animals, so we can use antibiotics that target those structures.
Protozoa don't have many properties that differ from our own cells'
properties, and human viruses work by hijacking our own cells to
reproduce themselves. In most cases we do not know of agents that harm
them without also harming us. This is why we don't have good (having
mild or no side-effects) antibiotic treatments for protozoal parasite
infections or virus infections.
Bacteriophage: a virus that must infect bacteria in order to reproduce itself. Synonym: phage.
The burst size of a phage is the average number of new phage produced by a single infected bacterium during the lytic growth cycle. This number varies widely for well-studied phages, from only a few to over one hundred.
Coliphage: a bacteriophage that infects E. coli.
A defective prophage is a prophage
that lacks some function(s) essential to viral reproduction. For
example, one or more essential genes might be missing or damaged. Toxin
genes present in such a DNA element may or may not be expressed to
produce active toxin, depending on how those genes are regulated and
where the phage defects are. A bacterium carrying a defective prophage
is not usually said to be a lysogen. Probably most bacterial genomes
contain fragments of one or more phage genomes, in various stages of
decay.
A eukaryote
is an organism containing subcellular compartments separated from the
cytoplasm by a lipid bilayer membrane. In particular the nucleus is so
contained in a separate compartment. Plants, animals, fungi, protozoa,
and algae are all eukaryotes.
A protein or gene family
is a set of proteins or genes that have sufficient similarity at the
amino acid or DNA sequence level that it appears they are evolutionarily
related. This is usually taken to mean that the different members of
the set function similarly and one can infer properties of a newly
recognized member from known properties of other members of the set.
G
H
Induction of a prophage
is an event in which the formerly quiescent genome of the phage becomes
activated and expresses the various genes necessary to the production
of new progeny phages. By this activation the phage enters the lytic
phase of its life cycle.
Although biologists argue about whether viruses are "alive", it is usual for phage biologists to speak of the life cycle
or life style or "growth" of the phage, in reference to the mode of
phage replication and exit from the infected cell once replication is
accomplished. The three alternatives recognized are
- a lytic infection in which replication of virus proceeds immediately and is followed by enzymatic destruction of the bacterial cell wall so that progeny viruses are released,
- a persistent infection in which replication of virus proceeds immediately and continuously, and progeny virions are extruded from the cell individually without compromising the physical integrity of the host bacterium, so that virus replication and bacterial replication can both continue, and
- a temperate life style in which following each phage infection of a bacterium the phage may choose between going ahead with a lytic infection or becoming established as a prophage in the host cell. In the prophage state the phage genome is mostly repressed and inactive, but at some later time can become reactivated (induced), whereupon a lytic or persistent infection ensues.
Illustrations
of phage life cycles (animated GIFs illustrating infection, the lytic
cycle, and the temperate life style use a tailed dsDNA phage example,
the persistent cycle example uses a ssDNA phage example). To view these
images please enable your browser for Java.
The adjective "lysogenic"
describes a bacterium as containing the genome of a bacterial virus
that is in the prophage state. Such a bacterium is said to be "a
lysogen", or said to be lysogenic for (name of the phage). See also temperate and prophage.
A moron
(in bacteriophage biology) is a DNA element inserted between a pair of
genes in one phage genome when the genes of this same pair are adjacent
in a related phage genome. The name derives from the fact that one phage
contains "more" DNA than the other at this particular spot (see
illustration 1). Many virulence factors of pathogenic bacteria are
actually encoded in the morons of integrated prophages (see illustration
2).
Illustrations for morons: to see larger versions of drawings please enable your browser for Java
N
An operon
is a cluster of adjacent genes that are all expressed from a single
promoter, generating a single mRNA transcript from which individual
proteins are translated. This type of gene organization is found only in
prokaryotic organisms and some viruses, as far as we know. It allows
coordinate regulation of all the genes in the cluster, and minimizes the
space needed for the genes. In bacteriophages, it is common for
specific groups of genes to be clustered in operons.
A pathogenicity island (PAI)
is a region of a bacterial chromosome that contains a cluster of
virulence factor genes associated with pathogenicity of that bacterium.
To be so designated the PAI must show internal (sequence) evidence that
the gene cluster has at some time in the past been horizontally
transferred from some other organism.
Pathovar:
Pathogenic variety. A group of subspecies of bacteria (all members of
the same species) that share a specific cluster of pathogenic behaviors.
Abbreviation: pv. Example: in bacteria that are pathogenic for plants
the designation is based on which type of plants are infected, such as Xanthomonas campestris pv. citri.
A bacteriophage is said to cause a persistent
infection when infection leads to virus replication but mature virions
are extruded individually from the host cell without killing the cell.
See life cycle.
Phage: a virus that must infect bacteria in order to reproduce itself. Synonym: bacteriophage.
Probiotic
is an adjective referring to a live microorganism product used to
protect or support the health of animals or people, usually by feeding
the organism orally. "Live cultures" in yogurt are an example. Modified
definitions are emerging as technology develops.
A prokaryote is an organism in which the genetic material is not
separated from the cytoplasm by a conventional lipid bilayer membrane.
The cells of these organisms do not separate their metabolic functions
into membrane-bounded compartments: although specialized membranes may
be present these are continuous extensions of the cytoplasmic membrane
that separates the cell from its environment. Known archaea and
virtually all known bacteria are prokaryotes (see also eukaryotes).
A prophage
is a bacterial virus the genome of which is residing in a bacterial
host in a passive state, not expressing many viral functions or
producing progeny virions. It may be incorporated into the bacterial DNA
or it may be a separately replicated molecule within the bacterial
cytoplasm. In some cases toxin genes present in prophage genomes have
gene expression signals that allow their independent function when the
viral genome is otherwise passive.
Q/R
Recombinant DNA is a term used specifically to mean DNA that has been linked enzymatically in the laboratory ("in vitro",
literal meaning "in glass") to DNA from a different cell, sometimes a
different type of organism, and then reintroduced into a living cell,
where the new combination of DNA sequences may give expression to
properties not observed in either of the contributing sources. Since
bacteriophages are in the business of carrying genetic information from
one bacterium to another, bacteriophage sequences are often used as a
carrier (usually termed "vector") to move other types of sequences
around in such procedures.
Respiratory burst,
also called "oxidative burst", refers to one of our bodily defense
mechanisms by which we fight microbial infections. The offending
microbes are engulfed by a type of blood cell called a "phagocyte",
where they are sequestered in an internal compartment called a
"phagolysosome". Here the microbes are attacked in various ways,
including by the cell producing, via their own metabolic activity, a
sudden increase in concentration (a burst) of highly reactive forms of
oxygen such as peroxides and superoxides. These oxygen radicals attack
and destroy microbial cells. Some pathogenic bacteria can protect
themselves against this type of attack by making enzymes, called
peroxidase and superoxide dismutase (Sod), that break down the oxygen
radicals into harmless products.
Serovar:
Serological variety. A subspecies (variety) of some pathogen that can
be specifically recognized by its behavior in some serological test
(literally: an immunological test conducted using serum), such as a test
for reaction with a particular antibody. Abbreviation: sv. Example: Salmonella enterica sv. typhimurium.
Shigatoxin can refer to a toxin produced either by bacteria in the genus Shigella, or by certain strains of E. coli such as O157:H7. When produced by E. coli, the toxin is sometimes referred to as a "shiga-like" toxin or as "Verotoxin". Shigatoxin is an A-B type toxin.
A bacteriophage is called temperate when it is capable of establishing a lysogenic
state in a susceptible bacterial host. This is a quiescent state in
which virus replication does not occur. If this option is not available
to the phage, the phage is referred to as "lytic" or sometimes as "virulent". See also life style.
Bacterial strains are called toxigenic
when they are capable of producing toxin. This terminology is typically
used to indicate that a bacterial (potential) pathogen is infected with
or lysogenic for a phage encoding toxin genes that are capable of
expression.
(1) In molecular biology a vector
is a set of bacteriophage or plasmid sequences that can be used to move
other DNA of interest, such as bacterial, human, or mouse genes, from
one organism to another during recombinant DNA procedures.
In general the vector DNA will have the properties that it can easily
be moved into and out of, and maintain itself, in the organism in which
we wish to study the DNA of interest. For example we might use
bacteriophage lambda DNA as a vector for replicating and studying
fragments of mouse DNA in the bacterium E. coli. (2) In medical microbiology a vector
is an intermediate host, often an insect, in which a pathogenic microbe
such as a bacterium or virus, can remain alive while being transferred
from a reservoir host to an alternate host. For example, in Lyme disease
the disease-causing bacteria Borrelia bergdorferi are
transferred among several hosts such as mouse, deer, and human, when a
tick takes a blood meal on one host, picking up the bacteria, and then
takes another blood meal in a different host, infecting that second
animal. The tick is said to a vector of Lyme disease.
Verotoxin, a synonym for shigatoxin, is so-called because this toxin can kill African green monkey kidney cells, also known as Vero cells.
A virulence factor
is a feature of a pathogenic organism that enhances its ability to
cause disease. This might be a structure, an enzyme, a transport system,
or any other cellular function that makes the bacteria more successful
in infecting some other organism. A PAI
that includes genes of some type known to be associated (in other
contexts) with phage is assumed to represent, at least in part, a
cryptic phage genome or genome fragment.
The adjective "virulent", (1) when
applied to a bacteriophage, means that infection of a bacterium by the
phage always proceeds to virus replication and lysis of the host (for
alternative phage life styles see life cycle). (2) When applied to a bacterium "virulent" means that the bacterium can cause disease in some animal or plant.
W/X/Y/Z
...............................................
Bacteriophages on the World Wide Web
Division M
[Division M is composed of researchers and teachers dedicated to the study of bacterial viruses]
Some links to sites elsewhere on the web that give information about bacteriophages.
Here
is a tiny selection from the many thousands of pages now on the web
with information about bacteriophages — these are sorted into the
categories:
- Research institutes, resource sites, & multi-group sites
- Phage pages from on-line course materials
- Sites of research groups & individual phage biologists
- Biotechnology companies
- Bacteriophage stock centers
- Odds 'n ends
Research institutes, resource sites, & multi-group sites
- All the Virology on the WWW
- Bacteriophage Ecology Group
- Virus Structure Resource/Fuller group
- NCBI/NLM linked list of bacteriophage genome sequences
- Georgian Academy of Sciences G. Eliava Institute of Bacteriophage, Microbiology, and Virology
- Indiana Biolab Bacteriophage Index
- International Committee on Taxonomy of Viruses (ICTV)
- Institute of Molecular Virology (IMV), University of Wisconsin at Madison
- Pittsburgh Bacteriophage Institute (PBI), University of Pittsburgh
- VIPER (Virus Particle Explorer) site at the Scripps Research Institute
- Web-based simulation of growth of bacteriophage T7. The site also has pages of general information about T7.
- X174 as the Protein Databank's Molecule of the Month
Phage pages from on-line course materials
- From a course of Alan Cann, University of Leicester, Bacteriophages
- From M. Hewlett Lambda lecture, Univ. of Arizona
- Evolved from S. Maloy's upper division course pages in Microbial Genetics
- S. Metzenberg, California State Univ., Northridge, lectures on phage vectors in Recombinant DNA Techniques
- From M. Mulligan, courses at Memorial University, Félix D'Herelle and the discovery of bacteriophage, lambda & M13 topics (1), (2), (3), and phage replication.
- Lambda Vectors from a Molecular Biology course At Drexel/Chemical Engineering
Research group sites with on-line phage information
|
|
Biotechnology companies interested in phage
Bacteriophage stock centers
- ATTC (American Type Culture Collection)
- MAFF (Ministry of Agriculture, Forestry, and Fisheries), Japan
- Pseudomonas Genetic Stock Center
- Several suppliers aimed at college and K12 teachers can provide inexpensive stocks of wild type bacteria and phage, and in some cases mutant strains if those are commonly used in teaching. These include
- Russell Knightley Media, commercial source of virus images
..............................
Major discoveries made with bacteriophages
Division M
[Division M is composed of researchers and teachers dedicated to the study of bacterial viruses]
• nature of a virus life cycle (one-step growth experiment: Ellis & Delbrück 1939, eclipse— phage T4: Doermann 1948,
• nature and types of genetic mutations (phage T1: the Luria & Delbrück fluctuation test (1) (2) 1943; Hershey & Luria, 1945) intracellular assembly— phage T2: Kellenberger 1962)
• confirmation that genes are made of DNA (phage T2: Hershey & Chase experiment, 1952)
• virus-mediated gene transfer between cells (now called “gene therapy” — phage P22, Zinder 1953)
• restriction and modification (phage : Bertani & Weigle, 1953. At the time, the phenomenon was called "host-controlled variation"), its enzymatic basis (bacteriophage P1: Dussoix & Arber, 1962)
• co-linearity of gene and protein (phage T4: Benzer, 1959)
• messenger RNA (phage T4: Brenner, Jacob, & Meselson, 1961)
• single-stranded DNA genome (phage X174: Sinsheimer, 1959)
• the nature of the genetic code (phage T4: Crick, Barnett, Brenner, & Watts-Tobin, 1961)
• physical nature of genetic recombination (phage : Meselson & Weigle 1961)
• chemical nature (protein) and mode of action (DNA binding) of a transcription factor (phage repressor— Jacob & Monod, 1961, Ptashne 1967)
• site-specific recombination (phage : Campbell 1962, Signer & Weil 1968, Echols, Gingery, & Moore 1968))
• DNA ligase (phage : Gellert 1967)
• important features of the mechanism of DNA replication (phage X174— in vitroDNA synthesis: Goulian, Kornberg, & Sinsheimer 1967, rolling circle: Gilbert & Dressler 1968;
phage T4— Okazaki fragments: Okazaki & Okazaki 1969;
phage M13— RNA primers: Brutlag, Schekman, & Kornberg 1971;
phage T7— visualization: Dressler, Magazin, & Wolfson 1972, completing ends of linear molecules: Watson 1972)
• anti-termination as a mechanism of transcriptional regulation ( : Roberts 1969)
• SDS-PAGE ( — first SDS gels: Weber & Osborn, 1969; phage T4— discontinuous buffer system: Laemmli, 1971; phage T7— slab gels: Studier, 1973)
• DNA cloning (phage : Berg, 1972, Lobban & Kaiser 1973)
• chaperonins (phage : Georgopoulos, Hendrix, Casjens, & Kaiser, 1973)
• characterization of insertion sequences& transposons ( — IS1: Hu, Otsubo, Davidson, & Saedler 1975
• overlapping genes (phage X174: Barrell, Air, & Hutchison, 1976)
• retroregulation as a mechanism of translational regulation ( : Guarneros & Galindo 1979)
• luciferase reporter phages for medical diagnostics (mycobacteriophages: Jacobs, Barletta, Udani, Chan, Kalkut, Sosne, Kieser, Sarkis, Hatfull, and Bloom 1993)
http://www.asm.org/division/m/blurbs/Secrets.html
.......................................
Lives At Risk From Drug-Resistant Bug.
By Greg Callagham
AUSTRALIA'S addiction to antibiotics has led to the spread in the community of a virulent new drug-resistant form of golden staph that is claiming its first lives, say infectious disease experts.
CA-MRSA (community-acquired methicillin-resistant staphylococcus aureus) targets young, healthy people with infections that can range from minor skin eruptions to loss of limbs and death, according to Peter Collignon, director of the infectious diseases unit at Canberra Hospital.
``If we don't do something to stop this bug from spreading, we're going to be hit on the back of the head,'' he said.
Professor Collignon estimates that there are 40,000 CA-MRSA infections per year in Australia -- and the number is rising rapidly. ``If only one per cent of these go really bad, that's 400 life-threatening cases per annum,'' he said.
Risk of infection is greatest among the young and active, as CA-MRSA is spread by direct skin-to-skin contact. Those involved in contact sports, some indigenous groups, gay men and prisoners are the most likely to get infected by CA-MRSA, but everyone is vulnerable, said Professor Collignon.
Classified early last century as among the deadliest of all disease-causing organisms, staphylococcus aureus lives on the skin or inside the nostrils of up to a third of Australians, and infections are up to 30 times more common than meningococcal disease. One of the three strains of CA-MRSA, most common on the eastern seaboard, can carry an antibiotic-resistant toxin called PVL that can kill within a matter of days.
With no national surveillance system of CA-MRSA or MRSA (the hospital-based form of the bug) in place, Professor Collignon says it's impossible to get a handle on the exact number of deaths or life-threatening infections. ``We can't get the federal Government to look at this,'' said Professor Collignon. ``This is a public health problem they don't want to deal with.'
'
A Killer in Our Midst -- The Weekend Australian Magazine
.........................
By Greg Callaghan
Only the afternoon before, this normally strong and fit boy had been shifting rocks on the family's idyllic rain forest enclave in Wondecla, 90km southwest of Cairns, with his older brother, Jack, mum and older sister, Terri. Just a couple of hours afterwards he complained of a tingling and burning sensation in his leg, upon which Vicky noticed a mysterious red rash rising up. Perhaps an insect bite, she thought. But as the night advanced, she suspected it was something far more troubling.
Once daylight broke, the 41-year-old mother, whose husband was away working in the mines in Papua New Guinea, wasted no time. She helped her son, now limping badly and deathly pale, into the family wagon for the 30-minute drive to the nearest hospital at Atherton. By the time he was admitted he was complaining of chest pain, had a fever of 40.3 degrees and his skin was breaking out in dark red, swollen pustules. Meningococcal disease, Vicky fretted. But a battery of blood tests revealed little more than an infection running out of control, and with Sean's condition deteriorating, baffled doctors transferred him to Cairns Base Hospital. There a doctor took a photograph of the rash engulfing his torso, scalp, face and ears.
After almost three days, with the microbe still unknown and medical options running out, Sean was airlifted to Mater Children's Hospital in Brisbane where he was immediately wheeled to intensive care, hooked up to a ventilator and drip-fed the antibiotic of last resort, vancomycin. Doctors put his chance of survival at 30 per cent. "There was so much infection in his lungs, says Vicky, "that his X-rays were white." With hope draining away she fell to her knees in the hospital chapel, "pleading with God not to take my baby away."
"I'd never heard of it," says Vicky. "I'd read about golden staph, but not MRSA or CA-MRSA." After continuing on high-dosage vancomycin, Sean began to make a slow but steady recovery. When he was discharged from hospital five weeks later, he had only 30 per cent lung capacity and was learning to walk again. Only now, four months later, is Sean anywhere near being the active boy he once was.
It turns out Sean is one of the lucky ones. Sydney teenager Reis Gray wasn't so fortunate. The strapping 190cm 17-year-old returned home from guitar lessons one Tuesday evening sniffling and feeling lethargic. The next day his mother, Julie, drove him to the local GP, who prescribed a course of antibiotics. When his colour didn't improve over the next 24 hours, a worried Julie phoned her mother, a retired nurse, but Reis insisted, "I'm fine, Mum. I don't feel any pain."
But he wasn't fine and on Friday morning Julie dragged him out of bed ("I just need to sleep," he moaned) and drove him to the GP, who took his pulse and immediately called an ambulance. Just before Reis was intubated in accident and emergency at Westmead Hospital, he asked, "Am I going to be all right, mum?"
"Of course you are, sweetheart," Julie replied without hesitation, genuinely believing that in a Sydney hospital in the 21st century, brimming with cutting-edge technology, that her healthy, outdoorsy son, who hadn't been in a hospital since he was born, would make a swift recovery. But it was to be the last time she heard Reis's voice.
Astonished doctors took one look at his X-rays and scheduled a double lung transplant - three-quarters of Reis's lung tissue was missing, eaten away by the bug. But before any transplant they had to halt the runaway infection in its tracks. They launched a barrage of antibiotics against it but the infection shook them all off like confetti.
This bright, gregarious young man - who enjoyed footy, fishing, and jamming with his dad, Warren, in the garage - never regained consciousness. Which didn't stop him battling his insidious assailant for 24 more days, until his heart finally gave out. "He was the baby of the family, the one who always made us laugh," says Julie, who has two older children, Josh, 20 and Jessica, 23. "He had his whole life ahead of him." In the middle of the dining table where we are talking, Reis smiles back at us from a white-framed photograph, a handsome young man with a lick of chestnut hair tumbling over his forehead. On a mantelpiece opposite stands a shiny wooden box. Inside rest his ashes.
YOU'VE HEARD ABOUT GOLDEN STAPH: go into hospital, come out sicker. Every year in Australia, this elusive microscopic foe infects at least 7000 patients, of whom about 2000 (or one-in-three) will die, a figure now exceeding the national road roll - and climbing. Every time you're opened up on the operating table or connected to a drip there's a risk staphylococcus aureus will slip into your bloodstream, making you sicker than you were before admission.
The form of staph you don't want to get is the one with the ungainly name, methicillan-resistant staphylococcus aureus, or MRSA, now immune to all but the most potent antibiotics. Get a serious MRSA infection and you'll be seriously ill; add it to a pre-existing condition and you may be fighting for your life. There isn't a hospital in Australia that hasn't had an outbreak of MRSA; it now represents up to a third of staph infections and it's become a massive problem in British and American hospitals. Sydneysider Alison Sayer, a victim of the 2005 terrorist attack in London, nearly lost her right foot - not to a bomb but to an MRSA infection she picked up while at St Mary's Hospital after surgery to repair her knee.
But MRSA has a new renegade cousin - one that hits you where you live. Community-acquired MRSA could be lurking on someone's hand when you shake it, their face when you kiss it, on a tea towel, on your computer keyboard, a piece of gym equipment, on a meeting room table. In short, you can catch it anywhere at any time. Those involved in contact sports or prone to cuts and scrapes, such as children, are at special risk.
Never heard of CA-MRSA? Neither have some GPs and nurses in Australia. It only popped up in a few isolated cases about 10 years ago in remote indigenous communities in Western Australia, the result of a lethal combination of poor hygiene, skin disease and the rampant overuse of antibiotics. But its three main strains have now spread through all our capital cities and, unlike the hospital variety, which mostly affects elderly and infirm patients, they prefer younger, fitter hosts. CA-MRSA is also much more easily transmitted and can be armed with the mother of all toxins, PVL, which can kill within a matter of days, usually from a necrotising infection that eats away at skin, bones and lungs.
In the US, strains of this savage little bug have struck down football players from the Cleveland Browns, the New England Patriots and the St Louis Rams, and forced trainers to disinfect equipment almost hourly. Schools have been temporarily shut down. All up, MRSA takes at least 90,000 lives in the US each year, making it a greater killer than AIDS and prompting headlines such as "the ticking time bomb." Stories abound on the internet of young people dying or becoming seriously ill and some sufferers have uploaded pictures of their gaping wounds on YouTube.
IT'S TEMPTING, OF COURSE, to toss CA-MRSA into the health-scare basket along with SARS, bird flu and mad cow disease. It's only when you listen to infectious disease specialists across the country that you realise this disease is likely to represent medicine's number-one nightmare in the next decade.
Declares John Turnidge, a professor of molecular science at the University of Adelaide: "CA-MRSA is the most lethal of the super-bugs. There's a Nobel Prize in this for whoever cracks the formula of beating it." Dr Peter Collignon, director of the infectious diseases unit at The Canberra Hospital, says: "If we don't do something to stop this bug from spreading, we're going to be hit on the back of the head". Keryn Christiansen, head of microbiology and infectious diseases at Royal Perth Hospital: "CA-MRSA isn't just a new problem - it's the biggest problem." Dr Graeme Nimmo, director of microbiology for Pathology Queensland: "Nothing like this has ever been seen. We're seeing more and more cases and it could erupt into an epidemic."
The odds of catching CA-MRSA are still low. But what's alarming the experts is how quickly it is spreading in Australia and how the epidemic is unfolding in the US. A study by Pathology Queensland found there was a sevenfold increase in cases over the past seven years. "Now that," says Nimmo, "is a major increase."
"We're seeing the first deaths," says Collignon, "and at Canberra Hospital we now have more infections from CA-MRSA than the hospital type. We need to stop it before it gains a foothold in the community." Some Sydney and Brisbane hospitals are reporting outpatients with CA-MRSA as many as three times a week.
Getting a handle on the number of CA-MRSA infections is devilishly difficult, because there isn't a national register of the hospital-dwelling MRSA, let alone the community-acquired one - a sore point with infectious-disease experts. At least a third of us, or about 8 million Australians, are walking around with golden staph up our noses, or crawling over our hands. For most, it's a silent, harmless passenger, one that may pop up in a minor infection such as a boil and be cleared with antibiotic cream. It's only when CA-MRSA goes helter-skelter in your bloodstream that it becomes life-threatening.
Mention the words "flesh-eating bug" and you immediately think of arms and legs turning black - meningococcal disease - but, in fact, staph-like complaints are at least 30 times more common. And unlike meningococcal, for which is there is a vaccine for the group C strain, staph-type infections continue to outwit doctors. "This is much bigger than meningococcal disease," says Turnidge. "Staphylococcus kills many more people than meningococci and we don't have a vaccine in the offing."
Babies are especially vulnerable - particularly if they are laid on shared furniture such as couches, where the bug can survive for up to six months. Disturbingly, a UK study found that 50 per cent of cot death victims had elevated levels of CA-MRSA, which can thrive in stale mattresses. The findings may explain why cot death, or sudden infant death syndrome, is more common in second and subsequent children. "This organism has tremendously good abilities to survive over long periods," says Collignon. "Mattresses shouldn't be used for more than one child."
Another recently noted trait of CA-MRSA has been its spread within families. Adelaide mother Annette Simpson*, her husband Joe and their two sons, James, six, and Ben, four, have all been struck with serious CA-MRSA skin infections. In January, James was hospitalized for the second time after the bacterium spread to his bones; it was only halted after a long course of IV antibiotics. "He fell off his bike on the Saturday, and on Sunday he couldn't walk," says Annette. Back in 2005, James developed a golf ball-sized boil on his left leg, which had to be surgically drained, and since then every member of the family has had at least one skin eruption of CA-MRSA. "I had one the size of a 50-cent piece on my backside,"; says Annette, who now wears latex gloves when handling food and cleaning. "We've learnt to go straight to hospital at the slightest sign of an infection."
WHEN DR JOHN MERLINO tilts a plastic petri dish teeming with 100 million CA-MRSA bacteria under a fluorescent light, it's easy to understand why it's nicknamed "golden staph. Five tiny antibiotic pills are immersed in a sea of golden particles; two have repelled the bacteria" (marked by a force field around them) and the remaining three are completely besieged (the antibiotics rendered impotent by the bug). In this culture - which Merlino orders up for any patient fighting an onslaught of antibiotic-resistant microbes - he can identify the drugs beating the bugs and those that have already surrendered.
"This is Darwinian survival of the fittest in action," says the 48-year-old microbiologist from Sydney's Concord Hospital. "All this microbe is trying to do is survive and reproduce, just like us." Overuse of antibiotics helps to breed hardier, stronger bugs in two ways, he explains. First, the laws of natural selection dictate that when a handful of bacteria survive a mass assault by antibiotics, they pass on their resistant genes to the next generation. Second, since antibiotics wipe out competing bacteria species, they leave a near-empty field for drug-resistant strains to thrive.
If this dish teeming with CA-MRSA were to burst over my hand suddenly and the bacterial invaders seep into my bloodstream via a small paper cut or sore, I'd start feeling crook within a matter of hours. Within 24 hours I'd be breaking out in vivid red, weeping sores, and feeling weak. Until this point a standard course of workhorse antibiotics might still wipe out the infection, but if it began to run rampant I'd be seriously ill with pneumonia within two or three days, at worst fighting off a bug that could be devouring my lungs at a rate of 15mm an hour. If heavy-duty IV antibiotics failed to arrest the infection it would all be over.
Or maybe I wouldn't get so much as a pimple or sniffle. My fate would depend on my physiological make-up, the strength of my immune system, and the bacterial load that enters my bloodstream. This is one of medicine's biggest mysteries: why is it that one person can walk around with a throat or hand full of disease-causing bacteria without getting sick but then transmit it to another who becomes mortally ill?
Scientists are convinced that it's not just our genetic make-up - the Human Genome Project identified a paltry 20,000 genes, not many more than it takes to make a fruit fly - but its chemical dance with the hordes of bacteria that make up our bodies, exceeding the total number of cells by about 10 to one.
A microbiologist for more than 20 years, Merlino is no alarmist. But he believes CA-MRSA is one bug we can't afford to take lightly. Even recent headlines and TV news stories about a new super-bug, VRE, or vancomycin-resistant enterococcus, worry him and other disease detectives far less than CA-MRSA. Why? Because in hospitals at least, the seawall against the rising tide of drug-resistant bugs is proper hand hygiene, the subject of a national campaign to be rolled out this year (the recent Garling inquiry in NSW strongly recommended sacking doctors who repeatedly failed to wash their hands).
Being in the outside world, CAMRSA is neither so easily controlled nor so selective about whom it strikes. What disturbs Merlino about the community strains of MRSA, he says, is that they have features allowing them to colonise skin more effectively than their hospital cousin.
For years, public health officials have been raising the alarm about how our over-reliance on antibiotics is breeding a generation of super-bugs increasingly resistant to the medicines designed to kill them. While our consumption of antibiotics has dropped, we are still the world's biggest net consumer after the number-one hypochondriac, France.
Studies now suggest that the more antibiotics you pop throughout your life, the more vulnerable you may be to infections such as CA-MRSA as you weed out susceptible germs but promote the growth of their hardier cousins. Adults are still given antibiotics for viral conditions such as colds or flu, even though the drugs are useless against viruses. Many of us stop taking the antibiotics when our symptoms go away but before an infection is completely cleared up, which allows the partially resistant microbes to flourish. And experts warn that too many antibiotics are fed to children for complaints that would have cleared up on their own.
Turnidge says he has been "rattling the antibiotic cage for over 20 years" but sees only inaction by governments. "Continuing high antibiotic use and the emergence of more resistant strains is a recipe for disaster," he warns. It's a simple numbers game, says Collignon, who believes we need to cut our consumption by 50 per cent or more. "If we use half the amount of antibiotics, the resistance to antibiotics will be halved." Antibiotics are precious drugs, he insists, "to be kept in reserve until we absolutely need them."
The age of antibiotics has given way to the age of anxiety, where drugs that once conquered everything from pneumonia to tuberculosis are losing their punch. Even vancomycin, whose name is derived from "vanquish," is struggling to fight the new mutating forms of MRSA. Consider this: the Centres for Disease Control in the US reports that the number of people dying from hospital infections jumped almost tenfold between 1992 and 2005 - from 13,300 to 100,000. Even worse, research into new antibiotics has been drastically neglected and underfunded for almost 30 years. "The money is in the pills you take for long periods, like those for blood pressure or depression. It's not in antibiotics, which you take for a brief period of time," laments Turnidge. Notes Christiansen: "For some organisms, we have absolutely nothing in the pipeline in the way of antibiotics, which is very troubling."
If there's nothing left to prescribe, where will we be? At worst, back to the days before penicillin became widely available in the mid-1940s, when staph infections had an almost 90 per cent mortality rate, when healthy young people such as Australian boxer Les Darcy (1895-1917) could die of complications from an infected tooth, and silent movie star Rudolph Valentino (1895-1926) from an infection after a perforated ulcer.
Already the war against antibiotic-resistant drugs is an increasing drain on the health-care system. At Royal Perth Hospital an outbreak of the killer superbug VRE in 2007 cost millions to eradicate in a sweeping "search and destroy" mission, says Christiansen. "We were successful in ridding the hospital of VRE - but it cost more than $2.7 million. That's one hospital and one outbreak of the disease."
There is some good news. In the US, scientists are developing a new class of antibiotics that targets a pair of enzymes the microbes depend on to copy their genes and reproduce. And mercifully, most cases of CA-MRSA are still susceptible to standard antibiotics. The hospital variety, meanwhile, is still responsive to powerful intravenous antibiotics such as vancomycin, linezolid and daptomycin. But the operative word here is "still". Most experts agree that we're losing the war against microbes and unless a breakthrough happens soon, the formidable barriers we have built against disease over the past 70 years will start falling down.
SO SLIPPERY A BUG IS CA-MRSA THAT even the most diligent hand-washing and surface sanitising are no guarantee against becoming infected, as Jan Skally, an intensive care nurse at Royal Perth Hospital, tragically found. Jan returned home from a concert late one Friday evening to find her 60-year-old husband Ed in bed, breathless and nauseous. He'd complained of feeling off colour the day before, but dismissed his sniffles and achiness as the first signs of a cold or flu. Jan checked his pulse and called a doctor, but as the clock ticked away it was apparent Ed was becoming worse. After dressing him and carrying him to the car, Jan drove to Royal Perth's emergency department, where Ed was wheeled into the high-dependency area.
At 4.30am Jan drove home to pick up a few things for Ed's hospital stay. She was gone for no more than an hour, but when she returned Ed had already been intubated and was being moved to intensive care. A bronchoscopy showed that Ed's lungs were riddled with holes and flooded with pus; a specialist described it as one of the most virulent pneumonias he'd ever seen. Ed didn't respond to a raft of antibiotics, including a dose of vancomycin, and suffered multiple organ failure within 24 hours. He died at 8am that Sunday.
Last month, Jan and Ed, the parents of two children in their late 20s, would have celebrated their 34th wedding anniversary. "I never got a chance to say goodbye," she says. "The last time I saw him smile was at the hospital, just before I returned home to grab the clothes, and I had no idea that this would happen. In all my years in intensive care, I'd never seen anyone deteriorate that fast."
When Jan first heard the letters MRSA from the specialist handling Ed, she imagined with horror that she may have infected him with the bug. However, it wasn't the hospital-borne pathogen that killed him but an outside strain, CA-MRSA, loaded with the telltale PVL toxin. "Where did he get it from?" she asks. "I don't know. I wash my hands constantly, not just in the hospital but when I'm at home."
Wherever Ed caught CA-MRSA, it's highly likely he passed it on to his wife, because three months after his death, Jan noticed a red boil on her thigh. She cleaned and dressed the wound but the infection spread within three days and her leg turned black between the knee and pelvis. Because she was a nurse, Jan had to be decontaminated with antiseptic washes and baths for 10 days, and only after 10 weeks of repeated testing was she allowed back into Royal Perth. "This is really the most frightening bug, "she says simply.
When you hear stories like this, what's a person to do? Certainly, doctors aren't suggesting avoiding hospital if you need an operation. Nor do they advocate refusing essential antibiotics to those who are seriously ill. It's more the casual dosing - for sore throats and mild infections (mostly caused by viruses, against which antibiotics are useless) - that create the problem. Staying clean and washing hands is a good protective measure but not foolproof. Ultimately, the best win will be a vaccine, but that's not even around the corner yet.
In the meantime Nimmo, Collignon, Christiansen and others are calling for MRSA and CA-MRSA to be made a notifiable disease Australia-wide. "We urgently need good national figures to keep tabs on how the infection is spreading," says Nimmo (so far, only in Western Australia is it mandatory for MRSA to be reported). "We can't get the Federal Government interested in this at all," says Collignon, who is worried about the "potentially catastrophic consequences" of CA-MRSA infiltrating the medical system and combining its genes with the hospital form of MRSA.
As a bacterium, CA-MRSA may still be in its youth, but evidence suggests it's growing up fast. "What we're looking at here," says Collignon, "is a strong, well-designed organism that's doing whatever it can to protect itself"
He pauses for a moment and then muses: "This is not going to go away."
______________________________
"* Not their real names. Senior editor Greg Callaghan's previous story was "Stadium rockers"(January 31-February 1).
,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,
Max F. Perutz Laboratories, University Departments at the Vienna Biocenter, Department of Microbiology and Genetics,1 InterCell AG, Vienna, Austria2
Received 16 February 2004/ Returned for modification 24 May 2004/ Accepted 8 June 2004
Bacteriophage therapy of bacterial infections has received renewed attention owing to the increasing prevalence of antibiotic-resistant pathogens. A side effect of many antibiotics as well as of phage therapy with lytic phage is the release of cell wall components, e.g., endotoxins of gram-negative bacteria, which mediate the general pathological aspects of septicemia. Here we explored an alternative strategy by using genetically engineered nonreplicating, nonlytic phage to combat an experimental Pseudomonas aeruginosa infection. An export protein gene of the P. aeruginosa filamentous phage Pf3 was replaced with a restriction endonuclease gene. This rendered the Pf3 variant (Pf3R) nonreplicative and concomitantly prevented the release of the therapeutic agent from the target cell. The Pf3R phage efficiently killed a wild-type host in vitro, while endotoxin release was kept to a minimum. Treatment of P. aeruginosa infections of mice with Pf3R or with a replicating lytic phage resulted in comparable survival rates upon challenge with a minimal lethal dose of 3. However, the survival rate after phage therapy with Pf3R was significantly higher than that with the lytic phage upon challenge with a minimal lethal dose of 5. This higher survival rate correlated with a reduced inflammatory response elicited by Pf3R treatment relative to that with the lytic phage. Therefore, this study suggests that the increased survival rate of Pf3R-treated mice could result from reduced endotoxin release. Thus, the use of a nonreplicating modified phage for the delivery of genes encoding proteins toxic to bacterial pathogens may open up a new avenue in antimicrobial therapy.
 Present address:
Institute for Food Science and Nutrition, Swiss Federal Institute of
Technology Zürich, 8092 Zürich, Switzerland.
Present address:
Institute for Food Science and Nutrition, Swiss Federal Institute of
Technology Zürich, 8092 Zürich, Switzerland.
............................
http://www.pnas.org/content/106/12/4629.full
In this work, we
engineered bacteriophage to overexpress proteins to target gene networks
to enhance bacterial killing by antibiotics. Phage therapy to kill
bacteria has been in use since the early 20th century (9). Phage can lyse bacteria or be modified to express lethal genes to cause cell death (10–14). However, phage that are directly lethal to their bacterial hosts can select for phage-resistant bacteria in a short time (10, 11, 15).
To reduce the development of phage resistance, we sought to develop
engineered phage that would exert minimal evolutionary pressures.
Instead of overexpressing lethal genes, our design targets nonessential
genes and the networks they regulate that are not directly attacked by
antibiotics. Combination therapy with different antibiotics, different
bacteriophage, or antibiotics plus phage may reduce the incidence of
phage resistance and/or antibiotic resistance (16–20).
Therefore, by using a combination of engineered antibiotic-enhancing
phage and antibiotics, we hoped to reduce the incidence of antibiotic
resistance and enhance bacterial killing
AUSTRALIA'S addiction to antibiotics has led to the spread in the community of a virulent new drug-resistant form of golden staph that is claiming its first lives, say infectious disease experts.
CA-MRSA (community-acquired methicillin-resistant staphylococcus aureus) targets young, healthy people with infections that can range from minor skin eruptions to loss of limbs and death, according to Peter Collignon, director of the infectious diseases unit at Canberra Hospital.
``If we don't do something to stop this bug from spreading, we're going to be hit on the back of the head,'' he said.
Professor Collignon estimates that there are 40,000 CA-MRSA infections per year in Australia -- and the number is rising rapidly. ``If only one per cent of these go really bad, that's 400 life-threatening cases per annum,'' he said.
Risk of infection is greatest among the young and active, as CA-MRSA is spread by direct skin-to-skin contact. Those involved in contact sports, some indigenous groups, gay men and prisoners are the most likely to get infected by CA-MRSA, but everyone is vulnerable, said Professor Collignon.
Classified early last century as among the deadliest of all disease-causing organisms, staphylococcus aureus lives on the skin or inside the nostrils of up to a third of Australians, and infections are up to 30 times more common than meningococcal disease. One of the three strains of CA-MRSA, most common on the eastern seaboard, can carry an antibiotic-resistant toxin called PVL that can kill within a matter of days.
With no national surveillance system of CA-MRSA or MRSA (the hospital-based form of the bug) in place, Professor Collignon says it's impossible to get a handle on the exact number of deaths or life-threatening infections. ``We can't get the federal Government to look at this,'' said Professor Collignon. ``This is a public health problem they don't want to deal with.'
'
A Killer in Our Midst -- The Weekend Australian Magazine
.........................
- A KILLER IN OUR MIDST
By Greg Callaghan
Its better known cousin evolved in
hospitals, but the latest super-bug can be picked up anywhere. Greg
Callaghan explains why infectious disease experts are calling CA-MRSA our biggest health challenge yet.
Sean Fisher couldn't see the armies of toxic bacteria deep inside his right thigh, killing off wave upon wave of white blood cells sent forth to defend him; he didn't know that a battalion of invaders was charging straight for his lungs, but the 10-year-old felt so ill he probably wouldn't have cared. He'd spent the night before vomiting violently and enduring painful cramps, cradled in the arms of his mother, Vicky, until dawn.
Sean Fisher couldn't see the armies of toxic bacteria deep inside his right thigh, killing off wave upon wave of white blood cells sent forth to defend him; he didn't know that a battalion of invaders was charging straight for his lungs, but the 10-year-old felt so ill he probably wouldn't have cared. He'd spent the night before vomiting violently and enduring painful cramps, cradled in the arms of his mother, Vicky, until dawn.
Only the afternoon before, this normally strong and fit boy had been shifting rocks on the family's idyllic rain forest enclave in Wondecla, 90km southwest of Cairns, with his older brother, Jack, mum and older sister, Terri. Just a couple of hours afterwards he complained of a tingling and burning sensation in his leg, upon which Vicky noticed a mysterious red rash rising up. Perhaps an insect bite, she thought. But as the night advanced, she suspected it was something far more troubling.
Once daylight broke, the 41-year-old mother, whose husband was away working in the mines in Papua New Guinea, wasted no time. She helped her son, now limping badly and deathly pale, into the family wagon for the 30-minute drive to the nearest hospital at Atherton. By the time he was admitted he was complaining of chest pain, had a fever of 40.3 degrees and his skin was breaking out in dark red, swollen pustules. Meningococcal disease, Vicky fretted. But a battery of blood tests revealed little more than an infection running out of control, and with Sean's condition deteriorating, baffled doctors transferred him to Cairns Base Hospital. There a doctor took a photograph of the rash engulfing his torso, scalp, face and ears.
After almost three days, with the microbe still unknown and medical options running out, Sean was airlifted to Mater Children's Hospital in Brisbane where he was immediately wheeled to intensive care, hooked up to a ventilator and drip-fed the antibiotic of last resort, vancomycin. Doctors put his chance of survival at 30 per cent. "There was so much infection in his lungs, says Vicky, "that his X-rays were white." With hope draining away she fell to her knees in the hospital chapel, "pleading with God not to take my baby away."
The head of intensive care, after receiving the results from a CT scan and further blood tests, rolled Sean on to his side to examine an abscess on his pelvis. Sean yelled in agony but the specialist had a diagnosis consisting of six strange letters: CA-MRSA, or community-acquired methicillin-resistant staphylococcus aureus, a new super-bug that lives not in hospital wards but in the outside world.
"I'd never heard of it," says Vicky. "I'd read about golden staph, but not MRSA or CA-MRSA." After continuing on high-dosage vancomycin, Sean began to make a slow but steady recovery. When he was discharged from hospital five weeks later, he had only 30 per cent lung capacity and was learning to walk again. Only now, four months later, is Sean anywhere near being the active boy he once was.
It turns out Sean is one of the lucky ones. Sydney teenager Reis Gray wasn't so fortunate. The strapping 190cm 17-year-old returned home from guitar lessons one Tuesday evening sniffling and feeling lethargic. The next day his mother, Julie, drove him to the local GP, who prescribed a course of antibiotics. When his colour didn't improve over the next 24 hours, a worried Julie phoned her mother, a retired nurse, but Reis insisted, "I'm fine, Mum. I don't feel any pain."
But he wasn't fine and on Friday morning Julie dragged him out of bed ("I just need to sleep," he moaned) and drove him to the GP, who took his pulse and immediately called an ambulance. Just before Reis was intubated in accident and emergency at Westmead Hospital, he asked, "Am I going to be all right, mum?"
"Of course you are, sweetheart," Julie replied without hesitation, genuinely believing that in a Sydney hospital in the 21st century, brimming with cutting-edge technology, that her healthy, outdoorsy son, who hadn't been in a hospital since he was born, would make a swift recovery. But it was to be the last time she heard Reis's voice.
Astonished doctors took one look at his X-rays and scheduled a double lung transplant - three-quarters of Reis's lung tissue was missing, eaten away by the bug. But before any transplant they had to halt the runaway infection in its tracks. They launched a barrage of antibiotics against it but the infection shook them all off like confetti.
This bright, gregarious young man - who enjoyed footy, fishing, and jamming with his dad, Warren, in the garage - never regained consciousness. Which didn't stop him battling his insidious assailant for 24 more days, until his heart finally gave out. "He was the baby of the family, the one who always made us laugh," says Julie, who has two older children, Josh, 20 and Jessica, 23. "He had his whole life ahead of him." In the middle of the dining table where we are talking, Reis smiles back at us from a white-framed photograph, a handsome young man with a lick of chestnut hair tumbling over his forehead. On a mantelpiece opposite stands a shiny wooden box. Inside rest his ashes.
YOU'VE HEARD ABOUT GOLDEN STAPH: go into hospital, come out sicker. Every year in Australia, this elusive microscopic foe infects at least 7000 patients, of whom about 2000 (or one-in-three) will die, a figure now exceeding the national road roll - and climbing. Every time you're opened up on the operating table or connected to a drip there's a risk staphylococcus aureus will slip into your bloodstream, making you sicker than you were before admission.
The form of staph you don't want to get is the one with the ungainly name, methicillan-resistant staphylococcus aureus, or MRSA, now immune to all but the most potent antibiotics. Get a serious MRSA infection and you'll be seriously ill; add it to a pre-existing condition and you may be fighting for your life. There isn't a hospital in Australia that hasn't had an outbreak of MRSA; it now represents up to a third of staph infections and it's become a massive problem in British and American hospitals. Sydneysider Alison Sayer, a victim of the 2005 terrorist attack in London, nearly lost her right foot - not to a bomb but to an MRSA infection she picked up while at St Mary's Hospital after surgery to repair her knee.
But MRSA has a new renegade cousin - one that hits you where you live. Community-acquired MRSA could be lurking on someone's hand when you shake it, their face when you kiss it, on a tea towel, on your computer keyboard, a piece of gym equipment, on a meeting room table. In short, you can catch it anywhere at any time. Those involved in contact sports or prone to cuts and scrapes, such as children, are at special risk.
Never heard of CA-MRSA? Neither have some GPs and nurses in Australia. It only popped up in a few isolated cases about 10 years ago in remote indigenous communities in Western Australia, the result of a lethal combination of poor hygiene, skin disease and the rampant overuse of antibiotics. But its three main strains have now spread through all our capital cities and, unlike the hospital variety, which mostly affects elderly and infirm patients, they prefer younger, fitter hosts. CA-MRSA is also much more easily transmitted and can be armed with the mother of all toxins, PVL, which can kill within a matter of days, usually from a necrotising infection that eats away at skin, bones and lungs.
In the US, strains of this savage little bug have struck down football players from the Cleveland Browns, the New England Patriots and the St Louis Rams, and forced trainers to disinfect equipment almost hourly. Schools have been temporarily shut down. All up, MRSA takes at least 90,000 lives in the US each year, making it a greater killer than AIDS and prompting headlines such as "the ticking time bomb." Stories abound on the internet of young people dying or becoming seriously ill and some sufferers have uploaded pictures of their gaping wounds on YouTube.
IT'S TEMPTING, OF COURSE, to toss CA-MRSA into the health-scare basket along with SARS, bird flu and mad cow disease. It's only when you listen to infectious disease specialists across the country that you realise this disease is likely to represent medicine's number-one nightmare in the next decade.
Declares John Turnidge, a professor of molecular science at the University of Adelaide: "CA-MRSA is the most lethal of the super-bugs. There's a Nobel Prize in this for whoever cracks the formula of beating it." Dr Peter Collignon, director of the infectious diseases unit at The Canberra Hospital, says: "If we don't do something to stop this bug from spreading, we're going to be hit on the back of the head". Keryn Christiansen, head of microbiology and infectious diseases at Royal Perth Hospital: "CA-MRSA isn't just a new problem - it's the biggest problem." Dr Graeme Nimmo, director of microbiology for Pathology Queensland: "Nothing like this has ever been seen. We're seeing more and more cases and it could erupt into an epidemic."
The odds of catching CA-MRSA are still low. But what's alarming the experts is how quickly it is spreading in Australia and how the epidemic is unfolding in the US. A study by Pathology Queensland found there was a sevenfold increase in cases over the past seven years. "Now that," says Nimmo, "is a major increase."
"We're seeing the first deaths," says Collignon, "and at Canberra Hospital we now have more infections from CA-MRSA than the hospital type. We need to stop it before it gains a foothold in the community." Some Sydney and Brisbane hospitals are reporting outpatients with CA-MRSA as many as three times a week.
Getting a handle on the number of CA-MRSA infections is devilishly difficult, because there isn't a national register of the hospital-dwelling MRSA, let alone the community-acquired one - a sore point with infectious-disease experts. At least a third of us, or about 8 million Australians, are walking around with golden staph up our noses, or crawling over our hands. For most, it's a silent, harmless passenger, one that may pop up in a minor infection such as a boil and be cleared with antibiotic cream. It's only when CA-MRSA goes helter-skelter in your bloodstream that it becomes life-threatening.
Mention the words "flesh-eating bug" and you immediately think of arms and legs turning black - meningococcal disease - but, in fact, staph-like complaints are at least 30 times more common. And unlike meningococcal, for which is there is a vaccine for the group C strain, staph-type infections continue to outwit doctors. "This is much bigger than meningococcal disease," says Turnidge. "Staphylococcus kills many more people than meningococci and we don't have a vaccine in the offing."
Babies are especially vulnerable - particularly if they are laid on shared furniture such as couches, where the bug can survive for up to six months. Disturbingly, a UK study found that 50 per cent of cot death victims had elevated levels of CA-MRSA, which can thrive in stale mattresses. The findings may explain why cot death, or sudden infant death syndrome, is more common in second and subsequent children. "This organism has tremendously good abilities to survive over long periods," says Collignon. "Mattresses shouldn't be used for more than one child."
Another recently noted trait of CA-MRSA has been its spread within families. Adelaide mother Annette Simpson*, her husband Joe and their two sons, James, six, and Ben, four, have all been struck with serious CA-MRSA skin infections. In January, James was hospitalized for the second time after the bacterium spread to his bones; it was only halted after a long course of IV antibiotics. "He fell off his bike on the Saturday, and on Sunday he couldn't walk," says Annette. Back in 2005, James developed a golf ball-sized boil on his left leg, which had to be surgically drained, and since then every member of the family has had at least one skin eruption of CA-MRSA. "I had one the size of a 50-cent piece on my backside,"; says Annette, who now wears latex gloves when handling food and cleaning. "We've learnt to go straight to hospital at the slightest sign of an infection."
WHEN DR JOHN MERLINO tilts a plastic petri dish teeming with 100 million CA-MRSA bacteria under a fluorescent light, it's easy to understand why it's nicknamed "golden staph. Five tiny antibiotic pills are immersed in a sea of golden particles; two have repelled the bacteria" (marked by a force field around them) and the remaining three are completely besieged (the antibiotics rendered impotent by the bug). In this culture - which Merlino orders up for any patient fighting an onslaught of antibiotic-resistant microbes - he can identify the drugs beating the bugs and those that have already surrendered.
"This is Darwinian survival of the fittest in action," says the 48-year-old microbiologist from Sydney's Concord Hospital. "All this microbe is trying to do is survive and reproduce, just like us." Overuse of antibiotics helps to breed hardier, stronger bugs in two ways, he explains. First, the laws of natural selection dictate that when a handful of bacteria survive a mass assault by antibiotics, they pass on their resistant genes to the next generation. Second, since antibiotics wipe out competing bacteria species, they leave a near-empty field for drug-resistant strains to thrive.
If this dish teeming with CA-MRSA were to burst over my hand suddenly and the bacterial invaders seep into my bloodstream via a small paper cut or sore, I'd start feeling crook within a matter of hours. Within 24 hours I'd be breaking out in vivid red, weeping sores, and feeling weak. Until this point a standard course of workhorse antibiotics might still wipe out the infection, but if it began to run rampant I'd be seriously ill with pneumonia within two or three days, at worst fighting off a bug that could be devouring my lungs at a rate of 15mm an hour. If heavy-duty IV antibiotics failed to arrest the infection it would all be over.
Or maybe I wouldn't get so much as a pimple or sniffle. My fate would depend on my physiological make-up, the strength of my immune system, and the bacterial load that enters my bloodstream. This is one of medicine's biggest mysteries: why is it that one person can walk around with a throat or hand full of disease-causing bacteria without getting sick but then transmit it to another who becomes mortally ill?
Scientists are convinced that it's not just our genetic make-up - the Human Genome Project identified a paltry 20,000 genes, not many more than it takes to make a fruit fly - but its chemical dance with the hordes of bacteria that make up our bodies, exceeding the total number of cells by about 10 to one.
A microbiologist for more than 20 years, Merlino is no alarmist. But he believes CA-MRSA is one bug we can't afford to take lightly. Even recent headlines and TV news stories about a new super-bug, VRE, or vancomycin-resistant enterococcus, worry him and other disease detectives far less than CA-MRSA. Why? Because in hospitals at least, the seawall against the rising tide of drug-resistant bugs is proper hand hygiene, the subject of a national campaign to be rolled out this year (the recent Garling inquiry in NSW strongly recommended sacking doctors who repeatedly failed to wash their hands).
Being in the outside world, CAMRSA is neither so easily controlled nor so selective about whom it strikes. What disturbs Merlino about the community strains of MRSA, he says, is that they have features allowing them to colonise skin more effectively than their hospital cousin.
For years, public health officials have been raising the alarm about how our over-reliance on antibiotics is breeding a generation of super-bugs increasingly resistant to the medicines designed to kill them. While our consumption of antibiotics has dropped, we are still the world's biggest net consumer after the number-one hypochondriac, France.
Studies now suggest that the more antibiotics you pop throughout your life, the more vulnerable you may be to infections such as CA-MRSA as you weed out susceptible germs but promote the growth of their hardier cousins. Adults are still given antibiotics for viral conditions such as colds or flu, even though the drugs are useless against viruses. Many of us stop taking the antibiotics when our symptoms go away but before an infection is completely cleared up, which allows the partially resistant microbes to flourish. And experts warn that too many antibiotics are fed to children for complaints that would have cleared up on their own.
Turnidge says he has been "rattling the antibiotic cage for over 20 years" but sees only inaction by governments. "Continuing high antibiotic use and the emergence of more resistant strains is a recipe for disaster," he warns. It's a simple numbers game, says Collignon, who believes we need to cut our consumption by 50 per cent or more. "If we use half the amount of antibiotics, the resistance to antibiotics will be halved." Antibiotics are precious drugs, he insists, "to be kept in reserve until we absolutely need them."
The age of antibiotics has given way to the age of anxiety, where drugs that once conquered everything from pneumonia to tuberculosis are losing their punch. Even vancomycin, whose name is derived from "vanquish," is struggling to fight the new mutating forms of MRSA. Consider this: the Centres for Disease Control in the US reports that the number of people dying from hospital infections jumped almost tenfold between 1992 and 2005 - from 13,300 to 100,000. Even worse, research into new antibiotics has been drastically neglected and underfunded for almost 30 years. "The money is in the pills you take for long periods, like those for blood pressure or depression. It's not in antibiotics, which you take for a brief period of time," laments Turnidge. Notes Christiansen: "For some organisms, we have absolutely nothing in the pipeline in the way of antibiotics, which is very troubling."
If there's nothing left to prescribe, where will we be? At worst, back to the days before penicillin became widely available in the mid-1940s, when staph infections had an almost 90 per cent mortality rate, when healthy young people such as Australian boxer Les Darcy (1895-1917) could die of complications from an infected tooth, and silent movie star Rudolph Valentino (1895-1926) from an infection after a perforated ulcer.
Already the war against antibiotic-resistant drugs is an increasing drain on the health-care system. At Royal Perth Hospital an outbreak of the killer superbug VRE in 2007 cost millions to eradicate in a sweeping "search and destroy" mission, says Christiansen. "We were successful in ridding the hospital of VRE - but it cost more than $2.7 million. That's one hospital and one outbreak of the disease."
There is some good news. In the US, scientists are developing a new class of antibiotics that targets a pair of enzymes the microbes depend on to copy their genes and reproduce. And mercifully, most cases of CA-MRSA are still susceptible to standard antibiotics. The hospital variety, meanwhile, is still responsive to powerful intravenous antibiotics such as vancomycin, linezolid and daptomycin. But the operative word here is "still". Most experts agree that we're losing the war against microbes and unless a breakthrough happens soon, the formidable barriers we have built against disease over the past 70 years will start falling down.
SO SLIPPERY A BUG IS CA-MRSA THAT even the most diligent hand-washing and surface sanitising are no guarantee against becoming infected, as Jan Skally, an intensive care nurse at Royal Perth Hospital, tragically found. Jan returned home from a concert late one Friday evening to find her 60-year-old husband Ed in bed, breathless and nauseous. He'd complained of feeling off colour the day before, but dismissed his sniffles and achiness as the first signs of a cold or flu. Jan checked his pulse and called a doctor, but as the clock ticked away it was apparent Ed was becoming worse. After dressing him and carrying him to the car, Jan drove to Royal Perth's emergency department, where Ed was wheeled into the high-dependency area.
At 4.30am Jan drove home to pick up a few things for Ed's hospital stay. She was gone for no more than an hour, but when she returned Ed had already been intubated and was being moved to intensive care. A bronchoscopy showed that Ed's lungs were riddled with holes and flooded with pus; a specialist described it as one of the most virulent pneumonias he'd ever seen. Ed didn't respond to a raft of antibiotics, including a dose of vancomycin, and suffered multiple organ failure within 24 hours. He died at 8am that Sunday.
Last month, Jan and Ed, the parents of two children in their late 20s, would have celebrated their 34th wedding anniversary. "I never got a chance to say goodbye," she says. "The last time I saw him smile was at the hospital, just before I returned home to grab the clothes, and I had no idea that this would happen. In all my years in intensive care, I'd never seen anyone deteriorate that fast."
When Jan first heard the letters MRSA from the specialist handling Ed, she imagined with horror that she may have infected him with the bug. However, it wasn't the hospital-borne pathogen that killed him but an outside strain, CA-MRSA, loaded with the telltale PVL toxin. "Where did he get it from?" she asks. "I don't know. I wash my hands constantly, not just in the hospital but when I'm at home."
Wherever Ed caught CA-MRSA, it's highly likely he passed it on to his wife, because three months after his death, Jan noticed a red boil on her thigh. She cleaned and dressed the wound but the infection spread within three days and her leg turned black between the knee and pelvis. Because she was a nurse, Jan had to be decontaminated with antiseptic washes and baths for 10 days, and only after 10 weeks of repeated testing was she allowed back into Royal Perth. "This is really the most frightening bug, "she says simply.
When you hear stories like this, what's a person to do? Certainly, doctors aren't suggesting avoiding hospital if you need an operation. Nor do they advocate refusing essential antibiotics to those who are seriously ill. It's more the casual dosing - for sore throats and mild infections (mostly caused by viruses, against which antibiotics are useless) - that create the problem. Staying clean and washing hands is a good protective measure but not foolproof. Ultimately, the best win will be a vaccine, but that's not even around the corner yet.
In the meantime Nimmo, Collignon, Christiansen and others are calling for MRSA and CA-MRSA to be made a notifiable disease Australia-wide. "We urgently need good national figures to keep tabs on how the infection is spreading," says Nimmo (so far, only in Western Australia is it mandatory for MRSA to be reported). "We can't get the Federal Government interested in this at all," says Collignon, who is worried about the "potentially catastrophic consequences" of CA-MRSA infiltrating the medical system and combining its genes with the hospital form of MRSA.
As a bacterium, CA-MRSA may still be in its youth, but evidence suggests it's growing up fast. "What we're looking at here," says Collignon, "is a strong, well-designed organism that's doing whatever it can to protect itself"
He pauses for a moment and then muses: "This is not going to go away."
______________________________
"* Not their real names. Senior editor Greg Callaghan's previous story was "Stadium rockers"(January 31-February 1).
© News Limited Australia. All rights reserved.
...........................................
Most of the patients in one cancer ward have a strain of vancomycin-resistant enterococcus, an antibiotic-resistant bacterium. That ward has 12 confirmed cases and there are 16 throughout the rest of the hospital. The bug is highly infectious and potentially fatal to vulnerable people.
The state's top infectious disease expert, Professor John Turnidge, said some patients would carry the bacteria with them when they moved to the proposed new RAH.
The State Government said the existing RAH facilities were not good enough for "optimum infection control" and said the new RAH's design - primarily single rooms - would help control the bug.
The Advertiser revealed last week wards had been placed into "lockdown".
Continued Page 4
RAH outbreak of highly infectious bug worsens
From Page 1
This means new patients are not being admitted.
Signs warning of the infection in wards D6 and C6 have been erected.
Those wards house longer-term, seriously ill patients who are most at risk from superbugs.
Professor Turnidge, who is SA Pathology's clinical director, said levels of VRE had been worsening because it was so highly contagious and the only way to slow the "epidemic" was by putting people in single rooms.
"This is certainly a very sticky organism that contaminates the environment (rather than just being spread from person to person)," he said. "You only have to be in the same room as someone to pick it up.
"The architecture of hospitals just does not lend itself to infection control," Professor Turnidge said. "The ideal hospital has all single rooms. That's the standard for the future."
When asked whether the promised single rooms at the proposed new RAH would help control the spread, he said patients would have to be quarantined once they were moved. "They'll bring it with them," he said.
"When you've got a greenfields site, you'll assume everyone from the old hospital has it.
"The challenge is to have enough single rooms to do that."
The Advertiser can reveal that a conference brief from the RAH's Infection Prevention and Control Unit, produced in October last year, warned the largest-ever outbreak of VRE had hit the state. The unit blamed the design of the "old hospital" and inadequate cleaning.
"Since January, 2008, 147 patients at the RAH have been detected with (the bacteria) in their stool," the unit's experts wrote.
"Although the majority are (relatively harmless) faecal colonisation, there have been six potentially life-threatening infections, including four bloodstream infections and two deep abscesses."
They warned most units in the hospital were affected. "Attempts to eradicate VRE have been hampered by the physical design of an old hospital with few single rooms and inadequate ablution facilities and the median three-day turnaround time for results of surveillance swabs."
The bug "colonises" the gut and is harmless in healthy people, but is dangerous in people with compromised immune systems, such as cancer patients.
A spokeswoman for Health Minister John Hill said steps had been taken to minimise the risk of VRE cross-infection.
"Currently, the majority of patients in the RAH are accommodated within multi-bed bays, with shared bathroom facilities and little opportunity for optimum infection control," the spokeswoman said.
"The new RAH will dramatically increase the number of single rooms, showers and toilets, providing patients with not only privacy and dignity, but also less risk of picking up infections during their stay."
SA Health's Central Northern Adelaide Health Service executive director Lesley Dwyer said there were increased levels of VRE at the RAH, so increased infection-control measures had been implemented.
The Australian Medical Association blamed the overuse of antibiotics for creating the superbugs.
((C) Copyright Nationwide News Pty Limited)
...........................................
BUG'S RIFE
RAH Superbug Outbreak Worsens
TORY SHEPHERD, HEALTH REPORTER
The Advertiser (Adelaide, Australia)
04-15-2009
Edition: 1 State
Section: News
A SUPERBUG infecting cancer patients at the Royal Adelaide Hospital is worsening because it cannot be eradicated in the ageing hospital.
Disease experts yesterday told The Advertiser the proposed $1.7 billion hospital to be built on the city railyards was the only hope of stopping the bug's spread.
A SUPERBUG infecting cancer patients at the Royal Adelaide Hospital is worsening because it cannot be eradicated in the ageing hospital.
Disease experts yesterday told The Advertiser the proposed $1.7 billion hospital to be built on the city railyards was the only hope of stopping the bug's spread.
Most of the patients in one cancer ward have a strain of vancomycin-resistant enterococcus, an antibiotic-resistant bacterium. That ward has 12 confirmed cases and there are 16 throughout the rest of the hospital. The bug is highly infectious and potentially fatal to vulnerable people.
The state's top infectious disease expert, Professor John Turnidge, said some patients would carry the bacteria with them when they moved to the proposed new RAH.
The State Government said the existing RAH facilities were not good enough for "optimum infection control" and said the new RAH's design - primarily single rooms - would help control the bug.
The Advertiser revealed last week wards had been placed into "lockdown".
Continued Page 4
RAH outbreak of highly infectious bug worsens
From Page 1
This means new patients are not being admitted.
Signs warning of the infection in wards D6 and C6 have been erected.
Those wards house longer-term, seriously ill patients who are most at risk from superbugs.
Professor Turnidge, who is SA Pathology's clinical director, said levels of VRE had been worsening because it was so highly contagious and the only way to slow the "epidemic" was by putting people in single rooms.
"This is certainly a very sticky organism that contaminates the environment (rather than just being spread from person to person)," he said. "You only have to be in the same room as someone to pick it up.
"The architecture of hospitals just does not lend itself to infection control," Professor Turnidge said. "The ideal hospital has all single rooms. That's the standard for the future."
When asked whether the promised single rooms at the proposed new RAH would help control the spread, he said patients would have to be quarantined once they were moved. "They'll bring it with them," he said.
"When you've got a greenfields site, you'll assume everyone from the old hospital has it.
"The challenge is to have enough single rooms to do that."
The Advertiser can reveal that a conference brief from the RAH's Infection Prevention and Control Unit, produced in October last year, warned the largest-ever outbreak of VRE had hit the state. The unit blamed the design of the "old hospital" and inadequate cleaning.
"Since January, 2008, 147 patients at the RAH have been detected with (the bacteria) in their stool," the unit's experts wrote.
"Although the majority are (relatively harmless) faecal colonisation, there have been six potentially life-threatening infections, including four bloodstream infections and two deep abscesses."
They warned most units in the hospital were affected. "Attempts to eradicate VRE have been hampered by the physical design of an old hospital with few single rooms and inadequate ablution facilities and the median three-day turnaround time for results of surveillance swabs."
The bug "colonises" the gut and is harmless in healthy people, but is dangerous in people with compromised immune systems, such as cancer patients.
A spokeswoman for Health Minister John Hill said steps had been taken to minimise the risk of VRE cross-infection.
"Currently, the majority of patients in the RAH are accommodated within multi-bed bays, with shared bathroom facilities and little opportunity for optimum infection control," the spokeswoman said.
"The new RAH will dramatically increase the number of single rooms, showers and toilets, providing patients with not only privacy and dignity, but also less risk of picking up infections during their stay."
SA Health's Central Northern Adelaide Health Service executive director Lesley Dwyer said there were increased levels of VRE at the RAH, so increased infection-control measures had been implemented.
The Australian Medical Association blamed the overuse of antibiotics for creating the superbugs.
((C) Copyright Nationwide News Pty Limited)
............................................
THREE more cases of an antibiotic-resistant
superbug have been identified at the Royal Adelaide Hospital and the
cause of the breakout identified.
South Australian chief medical officer Paddy Phillips said the number of infections was being revised constantly as tests were returned, but the hospital was looking at ways to control the outbreak.
"Patients who don't need to be admitted to the RAH (cancer ward) are not being admitted at the moment, it's being monitored on a daily basis and we're checking patients," he said.
He said the outbreak had been tracked back to two admissions a week ago, although their illnesses were not disclosed.
"There were two patients who came into hospital with diarrhoea and because the tests take several days, those people were in a multi-bed bay, and unfortunately other people became colonised (with the bug)," Professor Phillips said.
He could not confirm whether another ward had gone into lockdown to isolate the additional cases. Health Minister John Hill said he had been advised that this strain of bacteria, vancomycin-resistant enterococcus, was relatively common and was likely to exist in all SA hospitals. "I'm not aware of any particular incidents at the moment but I would be very surprised if they weren't in any other hospitals," he said.
Mr Hill said the incident was further evidence supporting the move to single-bed wards - as envisaged in the proposed $1.7 billion Royal Adelaide Hospital at City West.
"We have had this hospital for over 150 years and the only alternative is to keep it and fiddle around the issues or make a clean break and build a new hospital and that's what were going to do," he said.
But Save the RAH chairman Jim Katsaros said Mr Hill's argument was false.
"We only have 10 or 12 patients who are affected. It is bacteria in patients, and not in bricks," he said.
"A new hospital with 60 inpatients beds will not prevent on day one, 10 people with this bug walking through those doors and we will be back to square one."
..............................................
Netherlands based company, EBI Food Safety,
has announced that it has teamed up with US distributor World Technology
Ingredients (WTI) to accelerate the penetration of its GRAS approved phage
based product, Listex, into the North American meat and poultry sector.
Dirk de Meester, business development director at EBI, said that Listex received Generally Recognised as Safe (GRAS) approval by the US Food and Drug Administration (FDA) in 2006 for its use with cheese and was subsequently awarded GRAS affirmation in 2007 for use with all products that are susceptible to Listeria including hams, hot dogs, fish and ready-to-eat products.
He told FoodProductionDaily.com that as WTI has long standing relationships with North American meat and poultry processors as well as comprehensive technical expertise in the control of food pathogens, it is ideally placed to explain the benefits of Listex in this geography.
According to de Meester, Listex kills rather than inhibits the pathogen and in doing so does not affect the organolepetic properties of the food such as taste, texture, odour or colour, thus eliminating any requirement for the trade off between food safety and quality commonly associated with other methods of pathogen reduction.
He said that the phage based product is easy to apply, through spraying or submersion, and is used on meat products such as hot dogs after the post-lethality step; he said it is also recommended for use with fish after the filleting stage to prevent Listeria getting a hold.
Recall prevention
With the increasing emphasis by consumers and regulators on food safety, and the prospect of costly recalls, fines and brand damage, processors are constantly on the lookout for quicker and cheaper ways of preventing bacterial contamination of their products.
Canada’s outbreak of listeriosis last summer, which was linked to the deaths of 20 people, was traced to meats producer Maple Leaf’s plant near Toronto.
According to an analysis by Frost & Sullivan, phage technology is poised to become a food industry standard for ensuring products do not leave processing plants laden with dangerous pathogens.
Bacteriophages
Bacteriophages are natural micro organisms, but have been harnessed only recently for use to enhance food safety.
To food pathogens like Listeria, bacteriophages are the viral hit squads of the microscopic world. They are viruses that target bacteria, rather than human, plant or animal cells.
For every bacterium, there is a phage that likes to latch on to them, take over their life processes and multiply. The baby phages then burst out to attack other nearby targets, killing the host cell.
EBI Food Safety is also in the process of developing phages against pathogens such as Salmonella and Campylobacter, added de Meester.
Bug at RAH infects more
The Advertiser (Adelaide, Australia)
04-16-2009
Byline: RUSSELL EMMERSON, STATE POLITICAL REPORTER
Edition: 1 State
Section: News
South Australian chief medical officer Paddy Phillips said the number of infections was being revised constantly as tests were returned, but the hospital was looking at ways to control the outbreak.
"Patients who don't need to be admitted to the RAH (cancer ward) are not being admitted at the moment, it's being monitored on a daily basis and we're checking patients," he said.
He said the outbreak had been tracked back to two admissions a week ago, although their illnesses were not disclosed.
"There were two patients who came into hospital with diarrhoea and because the tests take several days, those people were in a multi-bed bay, and unfortunately other people became colonised (with the bug)," Professor Phillips said.
He could not confirm whether another ward had gone into lockdown to isolate the additional cases. Health Minister John Hill said he had been advised that this strain of bacteria, vancomycin-resistant enterococcus, was relatively common and was likely to exist in all SA hospitals. "I'm not aware of any particular incidents at the moment but I would be very surprised if they weren't in any other hospitals," he said.
Mr Hill said the incident was further evidence supporting the move to single-bed wards - as envisaged in the proposed $1.7 billion Royal Adelaide Hospital at City West.
"We have had this hospital for over 150 years and the only alternative is to keep it and fiddle around the issues or make a clean break and build a new hospital and that's what were going to do," he said.
But Save the RAH chairman Jim Katsaros said Mr Hill's argument was false.
"We only have 10 or 12 patients who are affected. It is bacteria in patients, and not in bricks," he said.
"A new hospital with 60 inpatients beds will not prevent on day one, 10 people with this bug walking through those doors and we will be back to square one."
..............................................
North American meat sector target of Listeria technology
Dirk de Meester, business development director at EBI, said that Listex received Generally Recognised as Safe (GRAS) approval by the US Food and Drug Administration (FDA) in 2006 for its use with cheese and was subsequently awarded GRAS affirmation in 2007 for use with all products that are susceptible to Listeria including hams, hot dogs, fish and ready-to-eat products.
He told FoodProductionDaily.com that as WTI has long standing relationships with North American meat and poultry processors as well as comprehensive technical expertise in the control of food pathogens, it is ideally placed to explain the benefits of Listex in this geography.
According to de Meester, Listex kills rather than inhibits the pathogen and in doing so does not affect the organolepetic properties of the food such as taste, texture, odour or colour, thus eliminating any requirement for the trade off between food safety and quality commonly associated with other methods of pathogen reduction.
He said that the phage based product is easy to apply, through spraying or submersion, and is used on meat products such as hot dogs after the post-lethality step; he said it is also recommended for use with fish after the filleting stage to prevent Listeria getting a hold.
Recall prevention
With the increasing emphasis by consumers and regulators on food safety, and the prospect of costly recalls, fines and brand damage, processors are constantly on the lookout for quicker and cheaper ways of preventing bacterial contamination of their products.
Canada’s outbreak of listeriosis last summer, which was linked to the deaths of 20 people, was traced to meats producer Maple Leaf’s plant near Toronto.
According to an analysis by Frost & Sullivan, phage technology is poised to become a food industry standard for ensuring products do not leave processing plants laden with dangerous pathogens.
Bacteriophages
Bacteriophages are natural micro organisms, but have been harnessed only recently for use to enhance food safety.
To food pathogens like Listeria, bacteriophages are the viral hit squads of the microscopic world. They are viruses that target bacteria, rather than human, plant or animal cells.
For every bacterium, there is a phage that likes to latch on to them, take over their life processes and multiply. The baby phages then burst out to attack other nearby targets, killing the host cell.
EBI Food Safety is also in the process of developing phages against pathogens such as Salmonella and Campylobacter, added de Meester.
...................................................
MICROSCOPIC DANGERS
The Advertiser (Adelaide, Australia)
04-17-2009
Byline: TORY SHEPHERD TORY SHEPHERD
Edition: 1 State
Section: Opinion
They are more powerful than modern medicine and are able to leap from patient to patient in a single day. They're superbugs, as TORY SHEPHERD reports.
ANTIBIOTICS kill bugs and save lives. They are one of the most important medical advances of the past century. But since penicillin and other antibiotics have started to be used widely, some bugs have started to build a resistance to them.
University of Adelaide biomedical expert Emeritus Professor Chris Burrell says over-prescription of antibiotics has led to the rise and rise of superbugs.
"In the minds of patients and the minds of GPs there's an expectation that the outcome of a consultation is going to be a pill," he says.
"GPs sometimes feel they're under pressure to prescribe an antibiotic."
The Australian Medical Association agrees, urging caution in the use of antibiotics to stop the proliferation of resistant strains.
It is a case of Darwin's theory of natural selection in action. The antibiotics kill off some vulnerable bacteria but leave a few resistant bacteria behind to grow and spread.
When those bacteria hit vulnerable people they can cause fatal infections and antibiotics are no longer of any use.
The most common superbug is methicillin resistant staphylococcus aureus, a form of golden staph. MRSA can get into the body through wounds or broken skin caused by surgery or other medical procedures.
The bug now infecting the Royal Adelaide Hospital - and potentially all our major hospitals - is vancomycin resistant enterococci, or VRE, a bug that is resistant to the antibiotic vancomycin.
As with MRSA, most people with VRE are not made sick by it. The bugs remain harmlessly in the gut.
But if someone who has had lots of antibiotics, has a serious disease, or a compromised immune system is infected with the bug, it can be very dangerous.
It can cause bloodstream infections, abscesses and death. And the problem is that it is, as SA Pathology clinical director Professor John Turnidge puts it, "very sticky".
WHILE most bugs spread from coughing, sneezing or contact, VRE can spread into the environment. It can cling to equipment, clothes and beds.
Even stringent hygienic measures struggle to control it.
Professor Turnidge says you only have to be in the same room as someone and you risk infection.
In crowded hospitals the problem is nigh impossible to control. Nurses have to change masks and gowns between patients, despite their already heavy workload. Signs throughout warn everyone to make liberal use of antiseptic gels - but it still spreads. Professor Burrell warns that if the superbugs continue to spread we are "right back where we were before we had penicillin. People have come to think that modern medicine should be able to protect us... so people are a bit surprised to find that we haven't got all the answers in this area," he says.
The best way to protect against the superbugs is with good hygiene and, on a broader level, by stopping the overuse of antibiotics.
The latest outbreak at the RAH began when two patients were put in a room with others and spread the bug. But it was already around anyway and the Government admits it is probably in other hospitals.
When The Advertiser revealed the present outbreak - now affecting about 30 people - the State Government immediately responded by pushing the benefits of its planned new RAH at the rail yards.
Experts, including Professor Turnidge, agree with the Government. They say single rooms, where people can be quarantined from each other, are the most effective way to control the contagion.
It may seem a convenient argument at a time when Health Minister John Hill is struggling to sell the idea of the new RAH to many, but it also makes sense, and many authorities agree modern facilities designed with infection control in mind are crucial to controlling the superbugs.
But the new RAH is still years away, so the story of the superbugs is not nearly finished and could well get worse before it is over.
And superbugs, particularly MRSA, are starting in some cases to spread into the community, an even more frightening scenario.
((C) Copyright Nationwide News Pty Limited)
They are more powerful than modern medicine and are able to leap from patient to patient in a single day. They're superbugs, as TORY SHEPHERD reports.
ANTIBIOTICS kill bugs and save lives. They are one of the most important medical advances of the past century. But since penicillin and other antibiotics have started to be used widely, some bugs have started to build a resistance to them.
University of Adelaide biomedical expert Emeritus Professor Chris Burrell says over-prescription of antibiotics has led to the rise and rise of superbugs.
"In the minds of patients and the minds of GPs there's an expectation that the outcome of a consultation is going to be a pill," he says.
"GPs sometimes feel they're under pressure to prescribe an antibiotic."
The Australian Medical Association agrees, urging caution in the use of antibiotics to stop the proliferation of resistant strains.
It is a case of Darwin's theory of natural selection in action. The antibiotics kill off some vulnerable bacteria but leave a few resistant bacteria behind to grow and spread.
When those bacteria hit vulnerable people they can cause fatal infections and antibiotics are no longer of any use.
The most common superbug is methicillin resistant staphylococcus aureus, a form of golden staph. MRSA can get into the body through wounds or broken skin caused by surgery or other medical procedures.
The bug now infecting the Royal Adelaide Hospital - and potentially all our major hospitals - is vancomycin resistant enterococci, or VRE, a bug that is resistant to the antibiotic vancomycin.
As with MRSA, most people with VRE are not made sick by it. The bugs remain harmlessly in the gut.
But if someone who has had lots of antibiotics, has a serious disease, or a compromised immune system is infected with the bug, it can be very dangerous.
It can cause bloodstream infections, abscesses and death. And the problem is that it is, as SA Pathology clinical director Professor John Turnidge puts it, "very sticky".
WHILE most bugs spread from coughing, sneezing or contact, VRE can spread into the environment. It can cling to equipment, clothes and beds.
Even stringent hygienic measures struggle to control it.
Professor Turnidge says you only have to be in the same room as someone and you risk infection.
In crowded hospitals the problem is nigh impossible to control. Nurses have to change masks and gowns between patients, despite their already heavy workload. Signs throughout warn everyone to make liberal use of antiseptic gels - but it still spreads. Professor Burrell warns that if the superbugs continue to spread we are "right back where we were before we had penicillin. People have come to think that modern medicine should be able to protect us... so people are a bit surprised to find that we haven't got all the answers in this area," he says.
The best way to protect against the superbugs is with good hygiene and, on a broader level, by stopping the overuse of antibiotics.
The latest outbreak at the RAH began when two patients were put in a room with others and spread the bug. But it was already around anyway and the Government admits it is probably in other hospitals.
When The Advertiser revealed the present outbreak - now affecting about 30 people - the State Government immediately responded by pushing the benefits of its planned new RAH at the rail yards.
Experts, including Professor Turnidge, agree with the Government. They say single rooms, where people can be quarantined from each other, are the most effective way to control the contagion.
It may seem a convenient argument at a time when Health Minister John Hill is struggling to sell the idea of the new RAH to many, but it also makes sense, and many authorities agree modern facilities designed with infection control in mind are crucial to controlling the superbugs.
But the new RAH is still years away, so the story of the superbugs is not nearly finished and could well get worse before it is over.
And superbugs, particularly MRSA, are starting in some cases to spread into the community, an even more frightening scenario.
((C) Copyright Nationwide News Pty Limited)
,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,
Therapy of Experimental Pseudomonas Infections with a Nonreplicating Genetically Modified Phage
Antimicrobial Agents and
Chemotherapy, October 2004, p. 3817-3822, Vol. 48, No. 10
0066-4804/04/$08.00+0 DOI: 10.1128/AAC.48.10.3817-3822.2004
Copyright © 2004, American Society for Microbiology. All Rights Reserved.
0066-4804/04/$08.00+0 DOI: 10.1128/AAC.48.10.3817-3822.2004
Copyright © 2004, American Society for Microbiology. All Rights Reserved.
Max F. Perutz Laboratories, University Departments at the Vienna Biocenter, Department of Microbiology and Genetics,1 InterCell AG, Vienna, Austria2
Received 16 February 2004/ Returned for modification 24 May 2004/ Accepted 8 June 2004
Bacteriophage therapy of bacterial infections has received renewed attention owing to the increasing prevalence of antibiotic-resistant pathogens. A side effect of many antibiotics as well as of phage therapy with lytic phage is the release of cell wall components, e.g., endotoxins of gram-negative bacteria, which mediate the general pathological aspects of septicemia. Here we explored an alternative strategy by using genetically engineered nonreplicating, nonlytic phage to combat an experimental Pseudomonas aeruginosa infection. An export protein gene of the P. aeruginosa filamentous phage Pf3 was replaced with a restriction endonuclease gene. This rendered the Pf3 variant (Pf3R) nonreplicative and concomitantly prevented the release of the therapeutic agent from the target cell. The Pf3R phage efficiently killed a wild-type host in vitro, while endotoxin release was kept to a minimum. Treatment of P. aeruginosa infections of mice with Pf3R or with a replicating lytic phage resulted in comparable survival rates upon challenge with a minimal lethal dose of 3. However, the survival rate after phage therapy with Pf3R was significantly higher than that with the lytic phage upon challenge with a minimal lethal dose of 5. This higher survival rate correlated with a reduced inflammatory response elicited by Pf3R treatment relative to that with the lytic phage. Therefore, this study suggests that the increased survival rate of Pf3R-treated mice could result from reduced endotoxin release. Thus, the use of a nonreplicating modified phage for the delivery of genes encoding proteins toxic to bacterial pathogens may open up a new avenue in antimicrobial therapy.
* Corresponding author.
Mailing address: Max F. Perutz Laboratories, University Departments at the
Vienna Biocenter, Department of Microbiology and Genetics, Dr. Bohrgasse 9/4,
1030 Vienna, Austria.
Phone: 43-1-4277-54609. Fax: 43-1-4277-9546. E-mail: Udo.Blaesi@univie.ac.at.
Antimicrobial Agents and
Chemotherapy, October 2004, p. 3817-3822, Vol. 48, No. 10
0066-4804/04/$08.00+0 DOI: 10.1128/AAC.48.10.3817-3822.2004
Copyright © 2004, American Society for Microbiology. All Rights Reserved.
This article has been cited by other
articles: 0066-4804/04/$08.00+0 DOI: 10.1128/AAC.48.10.3817-3822.2004
Copyright © 2004, American Society for Microbiology. All Rights Reserved.
- Lu, T. K., Collins, J. J.
(2009). Engineered bacteriophage targeting gene networks as adjuvants for
antibiotic therapy. Proc. Natl. Acad. Sci. USA 106: 4629-4634
[Abstract] [Full Text] - Williams, S. R., Gebhart,
D., Martin, D. W., Scholl, D. (2008). Retargeting R-Type Pyocins To
Generate Novel Bactericidal Protein Complexes. Appl. Environ.
Microbiol. 74: 3868-3876
[Abstract] [Full Text] - Scholl, D., Martin, D. W.
Jr. (2008). Antibacterial Efficacy of R-Type Pyocins towards Pseudomonas
aeruginosa in a Murine Peritonitis Model. Antimicrob. Agents
Chemother. 52: 1647-1652
[Abstract] [Full Text] - Heo, Y.-J., Chung, I.-Y.,
Choi, K. B., Lau, G. W., Cho, Y.-H. (2007). Genome sequence comparison and
superinfection between two related Pseudomonas aeruginosa phages, D3112
and MP22. Microbiology 153: 2885-2895
[Abstract] [Full Text] - Lu, T. K., Collins, J. J.
(2007). Dispersing biofilms with engineered enzymatic bacteriophage. Proc.
Natl. Acad. Sci. USA 104: 11197-11202
[Abstract] [Full Text] - Watanabe, R., Matsumoto,
T., Sano, G., Ishii, Y., Tateda, K., Sumiyama, Y., Uchiyama, J., Sakurai,
S., Matsuzaki, S., Imai, S., Yamaguchi, K. (2007). Efficacy of Bacteriophage
Therapy against Gut-Derived Sepsis Caused by Pseudomonas aeruginosa in
Mice. Antimicrob. Agents Chemother. 51: 446-452
[Abstract] [Full Text]
............................
http://www.pnas.org/content/106/12/4629.full
-
Edited by Arnold L. Demain, Drew University, Madison, NJ, and approved February 3, 2009 (received for review January 16, 2008)
Abstract
Antimicrobial drug development is increasingly lagging behind the evolution of antibiotic resistance, and as a result, there is a pressing need for new antibacterial therapies that can be readily designed and implemented. In this work, we engineered bacteriophage to overexpress proteins and attack gene networks that are not directly targeted by antibiotics. We show that suppressing the SOS network in Escherichia coli with engineered bacteriophage enhances killing by quinolones by several orders of magnitude in vitro and significantly increases survival of infected mice in vivo. In addition, we demonstrate that engineered bacteriophage can enhance the killing of antibiotic-resistant bacteria, persister cells, and biofilm cells, reduce the number of antibiotic-resistant bacteria that arise from an antibiotic-treated population, and act as a strong adjuvant for other bactericidal antibiotics (e.g., aminoglycosides and β-lactams). Furthermore, we show that engineering bacteriophage to target non-SOS gene networks and to overexpress multiple factors also can produce effective antibiotic adjuvants. This work establishes a synthetic biology platform for the rapid translation and integration of identified targets into effective antibiotic adjuvants.Keywords:- antibiotic adjuvants
- antibiotic resistance
- bacterial persistence
- bacteriophage therapy
- synthetic biology
Bacterial infections are responsible for significant morbidity and mortality in clinical settings (1).
Many infections that would have been cured easily by antibiotics in the
past now are resistant, resulting in sicker patients and longer
hospitalizations (1, 2).
The economic impact of antibiotic-resistant infections is estimated to
be between $5 billion and $24 billion per year in the United States (3).
Antibiotic resistance can be acquired genetically (e.g., via mutations
in antibiotic targets) or result from persistence, in which a small
fraction of cells in a population exhibits a non-inherited, phenotypic
tolerance to antimicrobials (1, 4, 5).
New classes of antibiotics and more effective antimicrobial agents are needed, but few are in pharmaceutical pipelines (1, 6).
High-throughput methodologies combined with traditional molecular
biology techniques have enabled the discovery of potential drug targets
for new antibiotics and antibiotic potentiators (7, 8).
However, translating these targets from identification to actual drug
compounds requires a significant amount of additional work and
investment. Moreover, antibiotic drugs typically do not take advantage
of targets that need to be up-regulated to achieve antimicrobial
activity. As a result, a significant gap remains between target
identification and drug development.
Results
Targeting the SOS DNA Repair System.
Bactericidal antibiotics (e.g., quinolones such as
ofloxacin) induce hydroxyl radical formation that leads to DNA, protein,
and lipid damage and ultimately to cell death (8). DNA damage induces the SOS response (21, 22), which results in DNA repair (Fig. 1A). It has been shown that bacterial killing by bactericidal antibiotics can be enhanced by knocking out recA and disabling the SOS response (8). Here we took an alternative approach and engineered M13mp18 phage to overexpress lexA3, a repressor of the SOS response (23). Overexpression of lexA to suppress the SOS system has been demonstrated to inhibit the emergence of antibiotic resistance (24).
We used M13mp18, a modified version of M13 phage, as our substrate,
because it is a non-lytic filamentous phage and can accommodate DNA
insertions into its genome (supporting information (SI) Fig. S1) (25).

............................................................................
Fig. 1.
Engineered ϕlexA3 bacteriophage enhances killing of wild-type E. coli EMG2 bacteria by bactericidal antibiotics. (A)
Schematic of combination therapy with engineered phage and antibiotics.
Bactericidal antibiotics induce DNA damage via hydroxyl radicals,
leading to induction of the SOS response. SOS induction results in DNA
repair and can lead to survival (8). Engineered phage carrying the lexA3 gene (ϕlexA3) under the control of the synthetic promoter PLtetO and an RBS (27) acts as an antibiotic adjuvant by suppressing the SOS response and increasing cell death. (B) Killing curves for no phage (black diamonds), unmodified phage ϕunmod (red squares), and engineered phage ϕlexA3 (blue circles) with 60 ng/ml ofloxacin (oflox) (solid lines, closed symbols). 108 pfu/ml phage was used. A growth curve for E. coli EMG2 with no treatment (dotted line, open symbols) is shown for comparison. ϕlexA3 greatly enhanced killing by ofloxacin by 4 h of treatment. (C) Killing curves for no phage (black diamonds), ϕunmod (red squares), and ϕlexA3 (blue circles) with 5 μg/ml gentamicin (gent). 109 pfu/ml phage was used. ϕlexA3 phage greatly increases killing by gentamicin. (D) Killing curves for no phage (black diamonds), ϕunmod (red squares), and ϕlexA3 (blue circles) with 5 μg/ml ampicillin (amp). 109 pfu/ml phage was used. ϕlexA3 phage greatly increases killing by ampicillin.
o repress the SOS response, we placed the lexA3 gene under the control of the synthetic PLtetO promoter followed by a synthetic ribosome-binding sequence (RBS) (8, 23, 26, 27); we named this phage ϕlexA3 (Figs. 1A and S1B) and the unmodified M13mp18 phage ϕunmod. PLtetO, which is an inducible promoter in the presence of the TetR repressor, is constitutively on in EMG2 cells, which lack TetR. PLtetO was used for convenience for our proof-of-concept experiments described here and would not necessarily be the promoter of choice in real-world situations. We confirmed that ϕlexA3 suppressed the SOS response induced by ofloxacin treatment by monitoring GFP fluorescence in E. coli K-12 EMG2 cells carrying a plasmid with an SOS-responsive promoter driving gfp expression (Fig. S2) (8).
To test ϕlexA3's antibiotic-enhancing effect, we obtained time courses for killing of E. coli
EMG2 bacteria with phage and/or ofloxacin treatment. We calculated
viable cell counts by counting cfus during treatment with no phage or
with 108 pfu/ml of phage and with no ofloxacin or with 60 ng/ml ofloxacin (Fig. 1B). Bacteria exposed only to ofloxacin were reduced by about 1.7 log10(cfu/ml) after 6 h of treatment, reflecting the presence of persisters not killed by the drug (Fig. 1B). By 6 h, ϕlexA3 improved the bactericidal effect of ofloxacin by 2.7 orders of magnitude compared with unmodified phage ϕunmod (≈ 99.8% additional killing) and by more than 4.5 orders of magnitude compared with no phage (≈ 99.998% additional killing) (Fig. 1B).
Unmodified phage enhanced ofloxacin's bactericidal effect, a finding
that is consistent with previous observations that unmodified
filamentous phage augment antibiotic efficacy against Pseudomonas aeruginosa (20). Other researchers have noted that M13-infected E. coli exhibited impaired host stress responses to conditions such as acid stress (28).
The mechanism by which unmodified filamentous phage can augment
antibiotic efficacy is not well characterized but may involve membrane
disruption or impaired stress responses. No significant bacterial
regrowth was apparent with combination phage and antibiotic treatment up
to 12 h (Fig. 1B) (10, 11, 15). We confirmed that both ϕunmod and ϕlexA3 replicated significantly during treatment (data not shown).
To test whether ϕlexA3 can act as an
antibiotic adjuvant in different situations, we assayed for bacterial
killing with varying initial phage inoculation doses (Fig. S3) and with varying doses of ofloxacin (Fig. S4) after 6 h of treatment, respectively. ϕlexA3 enhanced ofloxacin's bactericidal activity over a wide range of multiplicity of infection (MOI), from 1:1000 to 1:1 (Fig. S3). ϕlexA3's
ability to increase killing by ofloxacin at a low MOI reflects rapid
replication and infection by M13 phage. For ofloxacin concentrations of
30 ng/ml and higher, ϕlexA3 resulted in much greater killing compared with no phage or unmodified phage ϕunmod (Fig. S4). Thus, ϕlexA3 is a strong adjuvant for ofloxacin at doses below and above the minimum inhibitory concentration (60 ng/ml, data not shown).
We next determined whether our engineered phage could
increase killing by classes of antibiotics other than quinolones. We
tested ϕlexA3's antibiotic-enhancing effect for gentamicin, an aminoglycoside, and ampicillin, a β-lactam antibiotic. ϕlexA3 increased gentamicin's bactericidal action by more than 2.5 and 3 orders of magnitude compared with ϕunmod and no phage, respectively (Fig. 1C). ϕlexA3 also improved ampicillin's bactericidal effect by more than 2 and 5.5 orders of magnitude compared with ϕunmod and no phage, respectively (Fig. 1D). For both gentamicin and ampicillin, ϕlexA3's strong antibiotic-enhancing effect was noticeable after 1 h of treatment (Fig. 1 C and D). These results are consistent with previous observations that ΔrecA mutants exhibit increased susceptibility to quinolones, aminoglycosides, and β-lactams (8) and indicate that engineered phage such as ϕlexA3 can act as general adjuvants for the 3 major classes of bactericidal drugs.
We also found that engineered phage ϕlexA3
is capable of reducing the number of persister cells in populations
already exposed to antibiotics as well as enhancing antibiotic efficacy
against bacteria living in biofilms. For example, ϕlexA3
added to a population previously treated only with ofloxacin increased
the killing of bacteria that survived the initial treatment by ≈ 1 and
1.5 orders of magnitude compared with ϕunmod and no phage, respectively (Fig. S5). In addition, simultaneous application of ϕlexA3 and ofloxacin improved killing of biofilm cells by about 1.5 and 2 orders of magnitude compared with ϕunmod plus ofloxacin and no phage plus ofloxacin, respectively (Fig. S6).
Enhancing Killing of Antibiotic-Resistant Bacteria.
In addition to killing wild-type bacteria with increased
efficacy, engineered phage can enhance killing of bacteria that already
have acquired antibiotic resistance. We applied ϕlexA3 with ofloxacin against E. coli RFS289, which carries a mutation (gyrA111) that renders it resistant to quinolone antibiotics (7, 29). ϕlexA3 increased the bactericidal action of ofloxacin by more than 2 and 3.5 orders of magnitude compared with ϕunmod and no phage, respectively (Fig. 2).
These results demonstrate that antibiotic-enhancing phage can be used
to combat antibiotic-resistant bacteria and therefore may have the
potential to bring defunct antibiotics back into clinical use.
Fig. 2. Engineered ϕlexA3 bacteriophage enhances killing of quinolone-resistant E. coli RFS289 bacteria by ofloxacin. Killing curves for no phage (black diamonds), unmodified phage ϕunmod (red squares), and engineered phage ϕlexA3 (blue circles) with 1 μg/ml ofloxacin (oflox). 108 pfu/ml phage was used. ϕlexA3 greatly enhanced killing by ofloxacin by 1 h of treatment.

{kind=link}
{kind=link}
{kind=link}
,,,,,,,,,,,,,,,
Increasing Survival of Mice Infected with Bacteria.
To determine the clinical relevance of antibiotic-enhancing
phage in vivo, we tested the ability of our engineered phage with
ofloxacin to prevent death in mice infected with bacteria. Mice were
injected with E. coli EMG2 i.p. 1 h before receiving different i.v. treatments (Fig. 3A). Eighty percent of mice that received ϕlexA3 with ofloxacin survived, compared with 50% mice that received ϕunmod plus ofloxacin and 20% of mice that received ofloxacin alone (Fig. 3B).
The in vivo efficacy of our antibiotic-enhancing phage in rescuing
infected mice from death demonstrates the feasibility of our designs for
clinical use.

Fig. 3.
{kind=link}
{kind=link}
Fig. 3.
Engineered ϕlexA3 bacteriophage increases survival of mice infected with bacteria. (A) Female Charles River CD-1 mice were inoculated with i.p. injection of 8.8 * 107 cfu/mouse E. coli
EMG2 bacteria. After 1 h, the mice received no treatment or i.v.
treatment with 0.2 mg/kg ofloxacin plus no phage, plus unmodified phage ϕunmod, or plus engineered phage ϕlexA3 (109
pfu/mouse phage was used). The mice were observed for 5 days, and
deaths were recorded at the end of each day to generate survival curves.
[Mouse drawing reproduced under a Creative Commons Attribution 2.5
license (53).] (B) Survival curves for infected mice treated with phage and/or ofloxacin demonstrate that engineered phage ϕlexA3 plus ofloxacin (closed blue circles with solid line) significantly increases survival of mice compared with unmodified phage ϕunmod plus ofloxacin (closed red squares with solid line), no phage plus ofloxacin (closed black diamonds with solid line), or no treatment (open black diamonds with dashed line).
.....................
Reducing the Development of Antibiotic Resistance.

Discussion
View Abstract
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1168693
 This
article has been cited by other
articles in PMC.
This
article has been cited by other
articles in PMC.
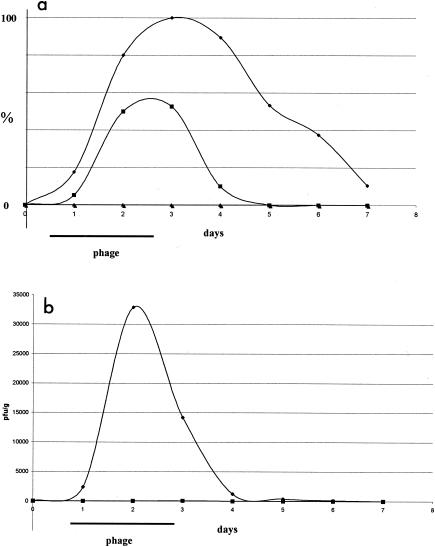
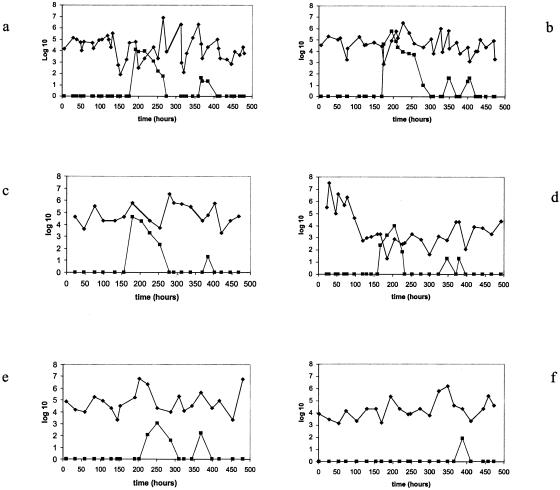
..............................................
Anthrax stopper
Travis, John
Science News
SCIENCE NEWS
This Week
Viral enzyme detects, kills bacterium
Last fall, envelopes full of anthrax-causing spores killed 5 people, sickened about a dozen, and struck fear in millions. Researchers funded by the U.S. military have now developed an innovative way to detect and kill Bacillus anthracis, the bacterium that causes anthrax. Seeking help from nature, the researchers are using an enzyme produced by a bacteriophage, a virus that preys upon bacteria.
The enzyme, called lysin, prevented the death of most mice that the researchers had infected with a bacterial relative of B. anthracis, Raymond Schuch of Rockefeller University in New York and his colleagues there report in the Aug. 22 Nature. The investigators also used the enzyme to create a prototype handheld instrument that quickly detects the anthrax bacterium, even in its spore form.
"This is avery clever exploitation" of lysin, says biowarfare researcher Stephen Morse of Columbia University.
Bacteriophages, or phages, infect bacteria in order to reproduce inside. Once they do, phages use lysin to break apart their hosts cell walls so the new phages can infect other bacteria "They cause the [bacterium] to explode," says study coauthor Vincent A. Fischetti.
Discovered nearly a century ago, bacteriophages have long attracted the interest of physicians seeking to control bacterial infections. Antibiotics stole the spotlight from phage therapy for many decades, but there's renewed interest in the strategy, given the rise of antibiotic-resistant bacteria (SN: 6/1/96, p. 350; 6/3/00, p. 358).
Over the past few years, Fischetti and his colleagues have exploited the bacteria-- killing talent of phages in a different way. They've shown that lysin itself represents a new way to destroy bacteria. For example, they've successfully used lysin to treat animals infected with bacteria that cause strep throat and pneumonia in people (SN: 6/10/00, p. 376).
Fischetti's group recently turned its attention to potential biowarfare agents, starting with the anthrax bacterium. While conventional antibiotics can treat many strains of B. anthracis, there's concern that resistant strains could evolve or be created, says Fischetti.
He and his colleagues began working with a phage that infects the anthrax bacterium almost exclusively and identified the gene encoding its lysin. In test-tube experiments, the enzyme destroyed strains ofB. anthracis collected from around the world but left most other bacteria unscathed.
Next, the scientists tested the enzyme on mice infected with a strain of Bacillus cereus closely related to the anthrax bacterium. This strain serves as an initial testing ground for anthrax therapies because B. anthracis is so dangerous to work with. The B. cereus strain typically kills infected mice, but treatment with lysin saved up to 76 percent of infected animals, Fischetti's team reports.
The researchers now plan to test the enzyme against B. anthracis, first in rodents and then in a nonhuman primate. If those experiments prove successfull, physicians would then assess the safety of the viral protein in human volunteers. If lysin passes muster, the U.S. and other governments could then consider stockpiling the enzyme for any future anthrax attack
Fischetti's group also built a B. anthracis detector. The investigators mixed lysin with chemicals that emit a flash of light when exposed to a substance released by dead bacteria. They also added an agent that induces B. anthracis spores to germinate, making them susceptible to lysin. Finally, they engineered a handheld light meter to monitor this broth and found it could detect a signal produced by as few as 100 spores within an hour of adding them to the broth.
"It's an innovative and promising strategy," says Morse.
.......................
THE NEXT PHAGE
Popular Science April 2009
How to heal an infection that defies antibiotics? Another infection. Doctors in Eastern Europe have used lab-grown viruses to safely cure millions of wounds. So why can't we do the same here?
It seemed like nothing at first. The red patch that appeared on Roy Brillon's thigh could have been a spider bite. But as the weeks passed, it grew and grew. By December 2004, the innocuous-looking bump had become an open wound the size of the palm of his hand. Brillon's doctor, Randy Wolcott, prescribed just about every antibiotic he could think of to cure the infection, but the lesion just got worse. "It was really bad," says Brillon, a 62-year-old retired housepainter from Lubbock, Texas. "I had to give up work because I couldn't climb ladders anymore."
Brillon felt like he was being eaten away from the inside out. And in a very real sense, he was. Left unchecked, bacteria like the streptococcus and staphylococcus devour soft tissue to keep themselves alive, leaving ragged red edges that expand outward with terrifying aggression. The pain in his leg was so excruciating that Wolcott prescribed morphine. "I was only supposed to take two pills a day, but I was taking three in the morning and three in the afternoon," he says. "The pain is indescribable. You just grit your teeth."
As head of Lubbock's Southwest Regional Wound Care Center, Wolcott knew well the typical prognosis for patients with antibiotic-resistant infections like Brillon's: gangrene, amputation and, for about 100,000 Americans a year, death. " 'Chronic wound' is a code word for 'you can't heal it,' " he says. "The hallmark is, we cut it off or we cut it out. It's pretty barbaric." Wolcott was desperate for an alternative. After putting in 10-hour days at the clinic, he often sat up late at night poring over medical journals for the newest wound-care research—something, anything that might help patients with the most intractable infections.
When Brillon arrived for a follow-up appointment three weeks later, Wolcott entered the room with a dropper in one hand and a vial of liquid that looked suspiciously like pond water in the other. The liquid, it turned out, was Wolcott's "anything": a murky concoction filled with bacteria-eating viruses known as bacteriophages. Physicians in Eastern Europe, Wolcott had explained to Brillon earlier, have been using phages safely since the 1920s to treat conditions that defy conventional antibiotics, from strep and tuberculosis to infected sores like his. Even U.S. drug companies sold them until the early 1940s, when penicillin came along and proved easier to use, generally more effective and, in the end, more lucrative than phages. The viruses might not help, he admitted, but if they didn't hurt, what was the harm in trying?
Brillon didn't need much convincing. The Food and Drug Administration was another story. Since 1963, the agency has mandated a strict approval process for all medications sold in America. Phage therapy has yet to be subjected to it, so Wolcott had to petition his state regulatory board to allow him to administer it only to people who had exhausted all other options. Then, because you can't find phages in U.S. pharmacies, he had to trek all the way to the former Soviet republic of Georgia to get it. There it's sold over the counter like eyedrops. He bought, for $2 each, three clear glass bottles, each filled with a liquid containing hundreds of types of phages.
"That's it?" Brillon asked, after Wolcott dribbled a few drops of the yellowish liquid onto his wound. The stuff was painless. Nothing much happened over the first few days, and Brillon braced himself for another disappointment. But as the week passed, the sore began to fade to a healthier pink, and then a new island of healthy skin emerged, expanding steadily every day. Within three weeks, the wound was completely healed. "You'd better take pictures of this," Brillon told Wolcott, "or nobody is going to believe it."
BRILLON'S RECOVERY was astonishing, but it wasn't a one-shot deal. Wolcott had also given the phage solution to 10 of his other worst-case patients, and many of them were showing similar results. If phages worked for them, Wolcott reasoned, couldn't they also work for the millions of patients in the U.S. living with infections resistant to antibiotics? His patients, he felt, were proof of it. The real question was whether he could convince the FDA.
As viruses go, phages are relatively benign. They're the most abundant naturally occurring organisms on Earth. They can be found virtually everywhere-in soil, drinking water, sewage. In fact, each one of us naturally has billions of them in our bodies. They prey only on bacteria, never human cells, they rarely spread from person to person, and, perhaps most important, bacteria have trouble becoming immune to them. As living organisms, phages are constantly changing and adapting in tandem with their host bacteria to kill them more effectively. Phage therapy could therefore eliminate the vicious cycle in which bacteria evolve resistance to antibiotics, necessitating the development of new, even more powerful drugs, at which point the process begins all over again.
But there's a big sticking point. The very characteristic that makes phages so effective-that expert ability to shape-shift- makes it difficult for them to pass muster with U.S. regulatory authorities. Although there have been no reports of adverse effects resulting from mutations, phages that don't normally nest inside the human body could potentially swap genes with other phages that do and produce foreign proteins that trigger an immune reaction. And it's impossible to say exactly how a virus might mutate when exposed to different bacteria, says Paul Sullam, a microbiologist at the University of California at San Francisco. For that reason, among others, says FDA spokesperson Karen Riley, phage therapy used to treat or cure humans must be regulated as a biological product. That means that if the viruses show serious signs of mutating or changing during clinical trials, even if those changes pose no risk to patients, the trials could be scrapped. Which explains why Big Pharma isn't eager to conduct them. "I understand where the FDA is coming from, because each phage poses a certain risk," Sullam says. "When viruses have the ability to exchange genetic material, it makes people nervous on a visceral level."
TO THE FDA, the serum Randy Wolcott drizzled on his patient's leg is new and unproven. But to the scientists working at the George Eliava Institute of Bacteriophage, Microbiology and Virology in the republic of Georgia, the medicine is as trusted as aspirin. Since 1923, when the facility was founded, scientists there have successfully treated millions of patients with phage therapy and presented more than 100 research abstracts at international conferences attesting to its clinical value.
Wolcott calls Eliava the "mother ship of phage research," a worldwide Mecca for people suffering from antibioticresistant infections. Only it doesn't look like the sort of place you'd want to go with a health problem. When Wolcott visited to hunt down alternatives for his patients, the four-story facility bore a closer resemblance to a neglected sanatorium. The walls were unpainted, the rooms were dark, and the equipment looked like museum pieces. "The conditions were abysmal," he says. "Yet the science is amazing."
Wolcott spent five days shadowing the staff and learning about phage therapy firsthand. "They had these 10-foot-tall fermenters, like big cooking pots, and they used them to make millions of doses of phage medication a year," he says. What surprised him most, aside from the dreary decor, was the painstaking way each prescription was custom-tailored for the patient. Phages are species-specific-different strains attack different bacteria. Since some wounds can harbor hundreds of different types of bacteria, physicians there first culture a tissue sample of the infection to determine its precise bacterial composition. The next step is to brew a custom cocktail of sometimes hundreds of phages selected from the institute's vast library of thousands. This whole process can take up to four days. The treatment-often administered through an IV bag that drips phage liquid directly into patients' wounds for 24 hours a day-can last up to two weeks.
As inconvenient as the procedure sounds, few people complain about it. The results are spectacular, Wolcott says: "I met a woman with a chronic ear infection who was coming back to the phage clinic for her final appointment. They gave her the therapy, and within a week, she was completely cleared up." In fact, studies published over the past several decades, based on trials conducted at Eliava and elsewhere in Eastern Europe, have shown that phage therapy has an 80 to 90 percent success rate against bacteria likely to show antibiotic resistance, such as Staphylococcus aureus and Escherichia coli. In contrast, many antibiotics fail outright against the evolved forms of these pathogens. In June 2005, a bacterial strain resistant to the first-line antibiotic imipenem ravaged more than 50 patients at New York City hospitals. Among patients whose infections infiltrated their bloodstream, the death rate was 47 percent.
With antibiotic resistance reaching record levels worldwide, phage therapy is no longer the sole province of Eastern European researchers. British biotech firm Biocontrol wrapped up the first Phase II clinical trial of phages in Western Europe last year with dramatic results. Its phage regimen combats the Pseudomonas aeruginosa bacterium, which causes serious lung and ear infections and is highly resistant to antibiotics. Patients with antibiotic-resistant infections who received phage therapy experienced a 50 percent reduction in their symptoms, compared with only a 20 percent decrease in the group that did not receive phages. "Frankly, I was blown away," says Dan Nelson, a biochemist at the University of Maryland who was at the conference where Biocontrol unveiled its results.
For Wolcott, who watches hundreds of patients die every year from seemingly incurable infections, these medicinal viruses can't arrive in the U.S. fast enough. "Phage needs to be fast-tracked. It works. It's completely natural. Why can't you spray this stuff on a kid's throat right now?"
IN TRUTH, phage therapy is already here, just not in a way that's practical for Wolcott. Owing to a regulatory technicality, manufacturers can use phages to keep ready-to-eat foods like deli meat and coleslaw safe from bacterial contamination, but doctors can't prescribe them to treat a bad case of strep. The difference, according to the FDA, is the application: Spraying a phage on lunch meat makes it a food additive. Give it to someone with an infection, and it becomes a drug. In 2006, the biotechnology company Intralytix took advantage of the less stringent regulatory rules for food additives to secure FDA clearance to sell a phage spray that kills Listeria bacteria, a common source of food poisoning. The company is also developing several phage treatments for humans, one of which entered clinical trials, thanks to Wolcott.
Wolcott met Intralytix CEO John Vazzana at a phage conference in Texas three months after he returned from Europe. The two talked for hours about the frustrating plight of phages in the U.S. By the end of the conference, they had hatched a plan to convince the FDA to let them start a clinical trial. Intralytix would supply the phages; Wolcott, the patients.
The FDA eventually agreed, on the condition that they limit the trial to only eight well-studied Intralytix phage strains. Wolcott quickly recruited 39 patients, all with infected venous leg ulcers, and set about conducting a two-year trial, the first of its kind on this side of the Atlantic.
Every week, Wolcott's study participants arrived at the clinic and received their phages through a handheld ultrasonic device, a high-tech upgrade to the IV drips common in Eastern Europe. The device simultaneously sprays on saline-based phage solution and destroys blackened or dead tissue, allowing the phages to penetrate deeper into the wound. Like all initial clinical trials, Wolcott's was designed to assess the safety of the therapy, not its outright effectiveness. In this context, the study yielded promising signs for the future. None of the patients in the trial reported severe side effects, but the efficacy was unimpressive. Nearly 70 percent of the volunteers experienced significant healing by the end of the 24-week trial period, as did a similar percentage of trial patients who did not receive the phage. Wolcott anticipated this, and attributes it to the fact that the cocktail was not tailored to combat the particular bacteria in his patients' wounds, as is standard practice in Georgia, limiting the phages' potency.
And this is where Wolcott hits a wall. FDA regulators have told him that if he wants to use phages on his patients, he's going to have to carry out a separate clinical trial for each phage or particular mix of phages he hopes to administer, just as he would if he were shepherding distinct chemical compounds through the regulatory process. But since each of his patients' wounds might contain hundreds of different species of bacteria, he can't reasonably attempt to conduct trials of the thousands of phage combinations required to combat them all, especially considering that the cost of a trial for a single drug can easily run into the millions. "People in this country have a right to be incensed that we have a very different situation here than in Europe with regards to phage," says Betty Kutter, a phage researcher at Evergreen State College. "Our whole regulatory environment has been one major thing that has slowed people down."
A Phase II efficacy trial enrolling 100 to 200 wound patients would cost about $9 million-and if the therapy being tested included only a few types of phages, as the first trial did, there's a good chance it wouldn't pan out for patients whose infections are caused by multiple strains of bacteria. And given the current regulations, Vazzana isn't sure he could even find the capital to fund the trial.
But phage researchers like Ben Burrowes of the Texas Tech University Health Sciences Center are optimistic. "Companies will start coming out with phage products at some point," he says, "and once those first few get through the approval process, the FDA will relax its standards a little."
RockefelleR university biologist Vincent Fischetti, for one, isn't holding his breath. Fischetti has no doubt that there's a gaping hole in the health-care landscape where effective antibacterial drugs should be. He just isn't sure phages are the best way to fill the void. To him, Wolcott and his fellow phage-therapy practitioners are like peacekeepers with no governmental backing: wellintentioned, to be sure, but unlikely to have much success in the end. "I'm not working on phage therapy," he insists, as he guides me through his sixth-floor lab overlooking the institute's Manhattan campus. "I'm working on phage-based therapy."
This distinction might seem arcane to nonbiologists, but in Fischetti's mind, it's a crucial one. While Wolcott sees phages as a major therapeutic coup, Fischetti sees them as merely an intermediate step toward a new generation of even better bacteria-fighters. He contends that the uphill regulatory battle phages face, as well as the risk of mutations, make them too big a gamble for American drug companies. "Phages are going to be a boutique treatment, nothing more," he says.
So he is taking an alternative approach, purifying the phage to extract the lysin, the enzyme it uses to dissolve the bacterial cell wall and kill the bacterium. He enlists his lab staff to serve as biological prospectors, collecting the bacteria-killing viruses from swamps, rivers, anywhere they can find them. He points to a bag of smelly bat excrement on his windowsill. "We can take the phages out of that stuff."
Having observed that lysins were the phages' "active ingredients," Fischetti aims to harvest the lysins from them and turn them into stable antibacterial drugs. If successful, he could accomplish a double feat previously thought impossible: getting the bacteria-fighting benefits of phages to patients, while doing an end run around the regulatory Rube Goldberg machine that researchers like Wolcott face.
Whereas phages must evolve to keep up with bacterial evolution, lysins are like a blunt instrument that can kill entire families of bacteria, eliminating the need to isolate and test thousands of different compounds as phage scientists in Georgia do. But even if the FDA might perceive lysins more favorably than phages alone, Kutter says, the enzymes have drawbacks of their own. Lysins work only on Gram-positive bacteria, like strep and staph, not Gram-negative bacteria like E. coli and salmonella-the Gram-negative bacteria have an outside membrane that the lysins can't get through. Phages, on the other hand, can work against both kinds of bacteria. And unlike traditional phage therapy, lytic enzymes haven't made it to clinical trials yet, so although petri-dish evidence is promising, there's no telling whether it will translate into success in a hospital setting.
It's clear that unless the FDA is willing to consider revised approval guidelines, phage therapy in the U.S. will remain in a holding pattern indefinitely. And in Lubbock, Roy Brillon's life has settled into a similar stasis. The phage Wolcott brought back from Georgia healed his leg wound, but since Brillon has problems with the valves that control blood flow in his leg veins, he's constantly developing new sores. "The blood goes down the veins, but it can't go back up," he explains. "The sores shrink and then pop up somewhere else on my leg."
What Brillon really needs, Wolcott says, is a phage cocktail custom-mixed to target the particular bacteria colonizing his wounds. But it's back to the same old antibiotics for now. Sometimes, if the bacteria happen to be non-drug-resistant, the antibiotics work; sometimes they yield about the same results as a newt's-eye potion. Brillon keeps his legs wrapped in Ace bandages like a burn victim. "If you don't keep 'em tight," he says, "then the legs swell, and that's when the sores come out."
But he's not dwelling on the obstacles. Instead he imagines the day when he'll be able to put his infections behind him for good and spend more time fishing and playing with his four grandchildren who live nearby. He figures that if anyone can get him there, it will be Wolcott and his army of phages. "It really bothers him if he gets ahold of something he can't handle," Brillon says. "He tells me, 'I'm never going to give up on you.' "
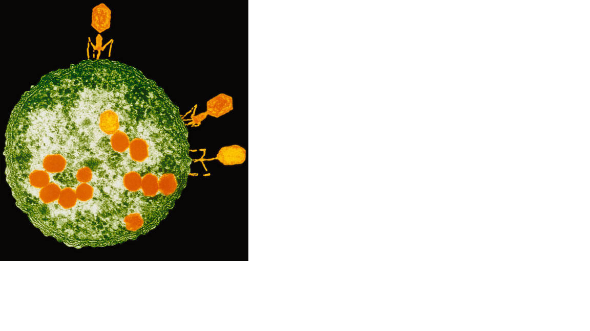
Elizabeth Svoboda is a contributing editor at Popular Science. Her last feature article, in July 2007, was about research efforts to turn algae into clean-burning biodiesel.
Copyright Bonnier Corporation Apr 2009
48 Hours; Dan Rather, Susan Spencer, Erin
Moriarty, Peter Van Sant
48 Hours (CBS) 09-20-2002
Environment
.....................
Reducing the Development of Antibiotic Resistance.
Exposure to subinhibitory concentrations of antibiotics can
lead to initial mutations that confer low-level antibiotic resistance
and eventually to more mutations that yield high-level resistance (30).
We hypothesized that engineered phage, as antibiotic adjuvants, could
reduce the number of antibiotic-resistant mutants that result from a
bacterial population exposed to antimicrobial drugs. To test this
hypothesis, we grew E. coli EMG2 in media with no ofloxacin for 24 h, with 30 ng/ml ofloxacin for 24 h, with 30 ng/ml ofloxacin for 12 h followed by ϕunmod plus ofloxacin treatment for 12 h, or with 30 ng/ml ofloxacin for 12 h followed by ϕlexA3 plus ofloxacin treatment for 12 h (Fig. S7).
Then, we counted the number of mutants resistant to 100 ng/ml ofloxacin
for each of the 60 samples under each growth condition. Growth in the
absence of ofloxacin yielded very few resistant cells (median = 1) (Fig. S7).
However, growth with subinhibitory levels of ofloxacin produced a high
number of antibiotic-resistant bacteria (median = 1592) (Fig. S7). Treatment with unmodified phage ϕunmod
decreased the number of resistant cells (median = 43.5); however, all
samples contained > 1 resistant cfu, and more than half of the
samples had > 20 resistant cfus (Fig. S7). In contrast, ϕlexA3
treatment dramatically suppressed the level of antibiotic-resistant
cells (median = 2.5), resulting in a majority of samples with either no
resistant cfus or < 20 resistant cfus (Fig. S7).
Flexible Targeting of Other Gene Networks.
Our phage platform can be used to target many different
gene networks to produce effective antibiotic adjuvants. To demonstrate
this feature, we engineered phage to express proteins that regulate
non-SOS gene networks (e.g., SoxR and CsrA) or modulate sensitivity to
antibiotics (e.g., OmpF) (Fig. 4 and Fig. S1) (27). For example, the soxRS regulon controls a coordinated cellular response to superoxide (31).
SoxR contains a [2Fe-2S] cluster that must be oxidized for it to
stimulate SoxS production, which then controls the transcription of
downstream genes that respond to oxidative stress (31). Because quinolones generate superoxide-based oxidative attack (7, 8), we surmised that engineering phage to overexpress wild-type SoxR (ϕsoxR) might affect this response and improve ofloxacin's bactericidal activity (Fig. 4A). As shown in Fig. 4B, ϕsoxR enhanced killing by ofloxacin compared with unmodified phage ϕunmod and no phage (Fig. 4B). However, the exact mechanism underlying the ability of SoxR overexpression in ϕsoxR
to enhance antibiotic killing is not clear. Overexpression of SoxR may
provide additional iron-sulfur clusters that could be destabilized to
increase sensitivity to bactericidal antibiotics (7, 8). Alternatively, because SoxR usually is kept at relatively low levels in vivo that are unchanged by oxidative stress (32),
overexpressing large amounts of SoxR may interfere with signal
transduction in response to oxidative stress by titrating intracellular
iron or oxidizing species or by competing with oxidized SoxR for binding
to the soxS promoter (32–34).
Reducing the Development of Antibiotic Resistance.
Exposure to subinhibitory concentrations of antibiotics can
lead to initial mutations that confer low-level antibiotic resistance
and eventually to more mutations that yield high-level resistance (30).
We hypothesized that engineered phage, as antibiotic adjuvants, could
reduce the number of antibiotic-resistant mutants that result from a
bacterial population exposed to antimicrobial drugs. To test this
hypothesis, we grew E. coli EMG2 in media with no ofloxacin for 24 h, with 30 ng/ml ofloxacin for 24 h, with 30 ng/ml ofloxacin for 12 h followed by ϕunmod plus ofloxacin treatment for 12 h, or with 30 ng/ml ofloxacin for 12 h followed by ϕlexA3 plus ofloxacin treatment for 12 h (Fig. S7).
Then, we counted the number of mutants resistant to 100 ng/ml ofloxacin
for each of the 60 samples under each growth condition. Growth in the
absence of ofloxacin yielded very few resistant cells (median = 1) (Fig. S7).
However, growth with subinhibitory levels of ofloxacin produced a high
number of antibiotic-resistant bacteria (median = 1592) (Fig. S7). Treatment with unmodified phage ϕunmod
decreased the number of resistant cells (median = 43.5); however, all
samples contained > 1 resistant cfu, and more than half of the
samples had > 20 resistant cfus (Fig. S7). In contrast, ϕlexA3
treatment dramatically suppressed the level of antibiotic-resistant
cells (median = 2.5), resulting in a majority of samples with either no
resistant cfus or < 20 resistant cfus (Fig. S7).
Flexible Targeting of Other Gene Networks.
Our phage platform can be used to target many different
gene networks to produce effective antibiotic adjuvants. To demonstrate
this feature, we engineered phage to express proteins that regulate
non-SOS gene networks (e.g., SoxR and CsrA) or modulate sensitivity to
antibiotics (e.g., OmpF) (Fig. 4 and Fig. S1) (27). For example, the soxRS regulon controls a coordinated cellular response to superoxide (31).
SoxR contains a [2Fe-2S] cluster that must be oxidized for it to
stimulate SoxS production, which then controls the transcription of
downstream genes that respond to oxidative stress (31). Because quinolones generate superoxide-based oxidative attack (7, 8), we surmised that engineering phage to overexpress wild-type SoxR (ϕsoxR) might affect this response and improve ofloxacin's bactericidal activity (Fig. 4A). As shown in Fig. 4B, ϕsoxR enhanced killing by ofloxacin compared with unmodified phage ϕunmod and no phage (Fig. 4B). However, the exact mechanism underlying the ability of SoxR overexpression in ϕsoxR
to enhance antibiotic killing is not clear. Overexpression of SoxR may
provide additional iron-sulfur clusters that could be destabilized to
increase sensitivity to bactericidal antibiotics (7, 8). Alternatively, because SoxR usually is kept at relatively low levels in vivo that are unchanged by oxidative stress (32),
overexpressing large amounts of SoxR may interfere with signal
transduction in response to oxidative stress by titrating intracellular
iron or oxidizing species or by competing with oxidized SoxR for binding
to the soxS promoter (32–34).

Fig. 4.
Engineered bacteriophage targeting
single and multiple gene networks (other than the SOS network) as
adjuvants for ofloxacin treatment (oflox). (A) Ofloxacin
stimulates superoxide generation, which normally is countered by the
oxidative stress response, coordinated by SoxR (8). Engineered phage producing SoxR (ϕsoxR) enhances ofloxacin-based killing by disrupting regulation of the oxidative stress response. (B) Killing curves for no phage (black diamonds), unmodified phage ϕunmod (red squares), and engineered phage ϕsoxR (blue downward-pointing triangles) with 60 ng/ml ofloxacin (solid lines, closed symbols). 108 pfu/ml phage was used. The killing curve for ϕunmod and a growth curve for E. coli EMG2 with no treatment (dotted line, open symbols) are reproduced from Fig. 1B for comparison and show that ϕsoxR enhances killing by ofloxacin. (C) CsrA suppresses the biofilm state in which bacterial cells tend to be more resistant to antibiotics (35). OmpF is a porin used by quinolones to enter bacterial cells (37). Engineered phage producing both CsrA and OmpF simultaneously (ϕcsrA-ompF)
enhances antibiotic penetration via OmpF and represses biofilm
formation and antibiotic tolerance via CsrA to produce an improved
dual-targeting adjuvant for ofloxacin. (D) Killing curves for ϕcsrA (black diamonds), ϕompF (red squares), and ϕcsrA-ompF (brown upward-pointing triangles) with 60 ng/ml ofloxacin. 108 pfu/ml phage was used. Phage expressing both csrA and ompF (ϕcsrA-ompF) is a better adjuvant for ofloxacin than phage expressing csrA (ϕcsrA) or ompF alone (ϕompF).
Fig. 4. {kind=link}
{kind=link}
CsrA is a global regulator of glycogen synthesis and
catabolism, gluconeogenesis, and glycolysis, and it also represses
biofilm formation (35). Because biofilm formation has been linked to antibiotic resistance, we hypothesized that csrA-expressing phage (ϕcsrA) would increase susceptibility to antibiotic treatment (Fig. 4C) (36). In addition, because OmpF is a porin used by quinolones to enter bacteria (37), we hypothesized that ompF-expressing phage (ϕompF) would increase killing by ofloxacin (Fig. 4C). After 6 h, both ϕcsrA and ϕompF increased ofloxacin's bactericidal effect by ≈ 1 and 3 orders of magnitude compared with ϕunmod and no phage, respectively (Fig. 4D).
Systems biology analysis often results in the
identification of multiple antibacterial targets that are not easily
addressed by traditional drug compounds. In contrast, engineered phage
are well suited for incorporating multiple targets into a single
antibiotic adjuvant. To demonstrate this capability, we designed an
M13mp18 phage to express csrA and ompF simultaneously (ϕcsrA-ompF) to target csrA-controlled gene networks and increase drug penetration (Fig. 4C) The multitarget phage was constructed by placing an RBS and ompF immediately downstream of csrA in ϕcsrA (Fig. S1F) (27). ϕcsrA-ompF was more effective in enhancing ofloxacin's bactericidal effect than were its single-target relatives, ϕcsrA and ϕompF, in planktonic (Fig. 4D) and biofilm (Fig. S8)
settings. Together, these results demonstrate that engineering phage to
target non-SOS genetic networks and/or overexpress multiple factors can
produce effective antibiotic adjuvants.
.......................................................Discussion
Our work demonstrates that combination therapy coupling
antibiotics with antibiotic-enhancing phage has the potential to be a
promising antimicrobial strategy. Moreover, we have shown that
antibiotic-enhancing phage should have clinical relevance because of
their in vivo effectiveness in rescuing infected mice. Thus, phage can
be engineered to act as effective antibiotic adjuvants in vitro and in
vivo and may help close the gap between antimicrobial target
identification and implementation. By targeting nonessential gene
networks, a diverse set of engineered bacteriophage can be developed to
supplement other antimicrobial strategies.
Despite the potential benefits described earlier in the
text, phage have yet to be accepted into clinical practice because of a
number of issues, such as phage immunogenicity, efficacy, target
bacteria identification and phage selection, host specificity, and toxin
release (9–11, 38, 39).
To reduce the risk of leaving lysogenic particles in patients after
treatment, our adjuvant phage could be modified to be nonreplicative, as
has been described previously (11).
A potential concern with the use of engineered M13mp18 prototype phage
described here is the development of phage resistance resulting from the
loss of the F-plasmid required for infection (10).
We have developed our prototype phage as a proof of concept for
antibiotic adjuvants and recognize that real-world usage may necessitate
the use of phage cocktails to ensure efficacy and the ability to treat
non-F-plasmid−containing bacteria. Phage cocktails that target
different, multiple bacterial receptors may reduce the development of
phage resistance by invading bacteria through different means. Using
phage cocktails with multiple antibiotics also could enhance bacterial
killing and reduce resistance to both phage and antibiotics.
Our phage platform for the development of effective
antibiotic adjuvants is a practical example of the application of
synthetic biology to important real-world biomedical issues. Synthetic
biology is focused on the rational and modular engineering of organisms
to create novel behaviors. The field has produced many reports of
synthetic gene circuits and systems with interesting characteristics (40–45). More recently, synthetic biologists have begun to address important industrial and medical problems (16, 46–48).
To extend our work beyond proof-of-concept experiments, libraries of
natural phage could be modified to target gene networks and pathways,
such as the SOS response, in different bacterial species (49, 50).
This process would require the isolation and genetic modification of
natural phage with the ability to infect the bacterial species being
targeted. With current DNA sequencing and synthesis technology, an
entire engineered bacteriophage genome carrying multiple constructs to
target different gene networks could be synthesized for less than
$10,000, a price that is sure to decrease in the future (51).
These technologies should enable large-scale modifications of phage
libraries to produce antibiotic-enhancing phage that can be applied with
different antibiotic drugs against a wide range of bacterial
infections. Targeting clinical bacterial strains with libraries of
engineered phage will be a crucial step in applying this strategy
against real-world infections.
Engineered phage may be adopted more readily in industrial,
agricultural, and food processing settings where bacterial biofilms and
other difficult-to-clear bacteria are present (16).
Applying engineered phage as antibiotic adjuvants in nonmedical
settings could be economically advantageous, reduce community-acquired
antibiotic resistance, and be a prudent first step toward gaining
acceptance for clinical use (52).
Materials and Methods
Bacterial Strains, Phage, and Chemicals.
E. coli K-12 EMG2 cells, which lack O antigens, were obtained from the Yale Coli Genetic Stock Center (CGSC #4401). E. coli RFS289 cells, which contain a gyrA111
mutation rendering them resistant to quinolones, were obtained from the
Yale Coli Genetic Stock Center (CGSC #5742). M13mp18 phage was
purchased from New England Biolabs. E. coli XL-10 cells used
for cloning, amplifying phage, and plating phage were obtained from
Stratagene. Chemicals were obtained from sources described in SI Materials and Methods.
Engineering M13mp18 Phage to Target Genetic Networks.
To construct engineered phage, lexA3, soxR, csrA, and ompF genes were first placed under the control of the PLtetO promoter in the pZE11G vector (23, 27). Details are described in SI Text. All PLtetO-gene constructs were followed by terminator T1 of the rrnB
operon and preceded by a stop codon; they were PCR amplified from the
respective pZE11 plasmids with primers 5′ aataca GAGCTC cTAA
tccctatcagtgatagagattg 3′ and 5′ taatct CGATCG tctagggcggcggat 3′ and
cloned into the SacI and PvuI sites of M13mp18 (Fig. S1) (25, 27).
Resulting phage genomes were transformed into XL-10 cells, mixed with
200 μl overnight XL-10 cells in 3 ml top agar, 1 mM isopropyl
β-D-1-thiogalactopyranoside (IPTG), and 40 μl of 20 mg/ml X-Gal, and
poured onto LB agar + chloramphenicol (30 μg/ml) plates for plaque
formation and blue-white screening. After overnight incubation of plates
at 37 °C, white plaques were scraped and placed into 1:10 dilutions of
overnight XL-10 cells and grown for 5 h. Replicative form (RF) M13mp18
DNA was collected by DNA minipreps of the bacterial cultures. All
insertions into M13mp18 were verified by PCR and restriction digests of
RF DNA. Infective phage solutions were obtained by centrifuging infected
cultures for 5 min at 16,100 × g and collecting supernatants followed by filtration through Nalge #190–2520 0.2 μm filters (Nalge Nunc International).
Determination of Plaque-Forming Units.
To obtain pfus, we added serial dilutions of phage
performed in 1X PBS to 200 μl of overnight XL-10 cells in 3 ml top agar,
1 mM IPTG, and 40 μl of 20 mg/ml X-Gal, and poured the mixture onto LB
agar + chloramphenicol (30 μg/ml) plates. After overnight incubation at
37 °C, plaques were counted.
Determination of Colony-Forming Units.
To obtain cfu counts, 150 μl of relevant cultures were
collected, washed with 1X PBS, recollected, and resuspended in 150 μl of
1X PBS. Serial dilutions were performed with 1X PBS and sampled on LB
agar plates. LB agar plates were incubated at 37 °C overnight before
counting.
Flow Cytometer Assay of SOS Induction.
To monitor ϕlexA3's suppression of the SOS response (Fig. S2), we used a plasmid containing an SOS-response promoter driving gfp expression in EMG2 cells (PLlexO-gfp) (7) with a basic protocol described in the SI Text.
Ofloxacin Killing Assay.
To determine the antibiotic-enhancing effect of engineered phage for ofloxacin (Figs. 1B, 4 B
and D), we grew 1:500 dilutions of EMG2 cells overnight for 3 h and 30
min at 37 °C and 300 rpm (model G25 incubator shaker; New Brunswick
Scientific) to late-exponential phase and determined initial cfus, which
were in the range of ≈ 109 cfu/ml. Then, we added 60 ng/ml ofloxacin alone or in combination with 108 pfu/ml phage (unmodified phage ϕunmod or engineered ϕlexA3, ϕsoxR, ϕcsrA, ϕompF, or ϕcsrA-ompF phage), and treated at 37 °C and 300 rpm. At indicated time points, we determined cfus as described earlier. Mean killing (Δlog10(cfu/ml)) was determined by subtracting mean initial log10(cfu/ml) from mean log10(cfu/ml) after treatment to compare data from different experiments. This protocol was replicated with E. coli RFS289 to determine the ofloxacin-enhancing effect of engineered ϕlexA3 phage against antibiotic-resistant bacteria (Fig. 2).
Dose–Response Assays.
The initial phage inoculation dose–response experiments (Fig. S3)
were conducted using the same protocol as the ofloxacin killing assay,
except that 60 ng/ml ofloxacin was added with varying concentrations of
phage. Cultures were treated for 6 h before obtaining viable cell
counts. The ofloxacin dose–response experiments (Fig. S4) also were obtained using the same protocol as in the ofloxacin killing assay, except that 108 pfu/ml phage was added with varying concentrations of ofloxacin, and viable cell counts were obtained after 6 h of treatment.
Gentamicin and Ampicillin Killing Assays.
To determine the antibiotic-enhancing effect of engineered
phage for gentamicin and ampicillin, we used the same protocol as in the
ofloxacin killing assay, except we used 109 pfu/ml initial phage inoculations. Five μg/ml gentamicin and 5 μg/ml ampicillin were used in Fig. 1 C and D, respectively.
Mouse Survival Assay.
Female Charles River CD-1 mice (weighing 18–20 g) received i.p. injections with 8.8 * 107 cfu/mouse E. coli EMG2 cells in a volume of 0.5 ml with 8% mucin (Fig. 3). After 1 h, the mice received either no treatment or i.v. infusions of ofloxacin alone (0.2 mg/kg), 109 pfu/mouse unmodified phage ϕunmod with ofloxacin (0.2 mg/kg), or 109 pfu/mouse engineered ϕlexA3phage
with ofloxacin (0.2 mg/kg). Ten mice were used per treatment group. The
mice were observed over 5 days, and deaths were recorded at the end of
each day. All mouse materials were provided by ViviSource Laboratories, a
facility approved by the United States Department of Agriculture and by
the Office of Laboratory Animal Welfare, where all in vivo experimental
work was performed.
Persister Killing Assay.
Persister killing (Fig. S5) was assayed using a basic protocol described in SI Text.
Biofilm Killing Assay.
Biofilm killing (Fig. S6 and Fig. S8) was assayed using a previously reported protocol described in SI Text (16).
Antibiotic Resistance Assay.
To analyze the effect of subinhibitory concentrations of
ofloxacin on the development of antibiotic-resistant mutants, we grew
1:108 dilutions of EMG2 cells overnight in LB media containing either no ofloxacin or 30 ng/ml ofloxacin (Fig. S7).
After 12 h of growth at 37 °C and 300 rpm (model G25 incubator shaker,
New Brunswick Scientific), we split the cells grown in no ofloxacin into
100-μl aliquots with no ofloxacin into 60 wells in 96-well plate format
(Costar 3370; Fisher Scientific). We also split the cells grown in 30
ng/ml ofloxacin into 100-μl aliquots in 60 wells with no phage and 30
ng/ml ofloxacin, with ϕunmod and 30 ng/ml ofloxacin, or with ϕlexA3
and 30 ng/ml ofloxacin in 96-well plates. We placed the 96-well plates
in 37 °C and 300 rpm with plastic bags to minimize evaporation. After 12
h of treatment, we plated cultures from each well on LB agar + 100
ng/ml ofloxacin to select for mutants that developed resistance against
ofloxacin. To compare results, we constructed box-and-whisker plots
using the 60 individual observations for each treatment condition (Fig. S7).
Statistical Analysis.
All cfu data were log10-transformed before
analysis. For all data points in all experiments, 3 samples were
collected except where noted. Error bars in figures indicate standard
error of the mean.
Acknowledgments
We thank Andrew Slee and Tim Murphy from ViviSource
Laboratories for their assistance with our in vivo mouse studies. We
greatly appreciate the reviewers' critique of our research. This work
was supported by the National Institutes of Health Director's Pioneer
Award Program (Grant DP1 OD00344), the National Science Foundation
Frontiers in Integrative Biological Research Program, and the Howard
Hughes Medical Institute. T.K.L. was supported by a Howard Hughes
Medical Institute Predoctoral Fellowship and a Harvard-MIT Health
Sciences and Technology Medical Engineering/Medical Physics Fellowship.
Footnotes
- 1To whom correspondence should be addressed. E-mail: jcollins@bu.edu
-
Author contributions: T.K.L. and J.J.C. designed research; T.K.L. performed research; T.K.L. contributed new reagents/analytic tools; T.K.L. analyzed data; and T.K.L. and J.J.C. wrote the paper.
-
Conflict of interest statement: We have submitted a patent disclosure regarding the work described in this paper.
-
This article is a PNAS Direct Submission.
-
This article contains supporting information online at www.pnas.org/cgi/content/full/0800442106/DCSupplemental.
-
Freely available online through the PNAS open access option.
References
................
Copyright © 2005,
American Society for Microbiology
Human Volunteers Receiving Escherichia coli Phage
T4 Orally: a Safety Test of Phage Therapy
Anne Bruttin and Harald Brüssow*
Nestlé Research
Center, Nestec Ltd., Vers-chez-les-Blanc, CH-1000 Lausanne 26, Switzerland
*Corresponding author. Mailing address:
Nestlé Research Center, Nestec Ltd., Vers-chez-les-Blanc, CH-1000 Lausanne 26, Switzerland.
Phone: 41 21 785 86 76. Fax: 41 21 785 85 49. E-mail: harald.bruessow@rdls.nestle.com .
Received November 25, 2004;
Revised January 24, 2005; Accepted April 3, 2005.
Abstract
Fifteen healthy adult volunteers
received in their drinking water a lower Escherichia coli phage T4 dose
(103 PFU/ml), a higher phage dose (105 PFU/ml), and
placebo. Fecal coliphage was detected in a dose-dependent way in volunteers
orally exposed to phage. All volunteers receiving the higher phage dose showed
fecal phage 1 day after exposure; this prevalence was only 50% in subjects
receiving the lower phage dose. No fecal phage was detectable a week after a
2-day course of oral phage application. Oral phage application did not cause a
decrease in total fecal E. coli counts. In addition, no substantial
phage T4 replication on the commensal E. coli population was observed.
No adverse events related to phage application were reported. Serum
transaminase levels remained in the normal range, and neither T4 phage nor
T4-specific antibodies were observed in the serum of the subjects at the end of
the study. This is, to our knowledge, the first safety test in the recent
English literature which has measured the bioavailability of oral phage in
humans and is thus a first step to the rational evaluation of phage therapy for
diarrheal diseases.
Antibiotic treatment of Escherichia
coli diarrhea is frequently problematic, which raises interest in
alternative approaches. Felix d'Hérelle, the codiscoverer of phages, advocated
the idea of exploiting the lytic effect of phages on bacteria for therapeutic
purposes. Phage therapy has a colorful history but became a common therapy for
intestinal and skin infections only in the Soviet Union
(17).
Currently, we see a renewed interest in phage therapy (13).
The present study describes the oral administration of phages to human
volunteers and the subsequent clinical and microbiological analyses. This
safety test is a follow-on from ecology studies of T4-like phages isolated from
the stools of pediatric diarrhea patients (7),
the analysis of their genomes (6),
and their behavior in experimental animals (8).
MATERIALS AND METHODS
Subjects.
Fifteen healthy adult volunteers
between 23 and 54 years of age (six women and nine men) were recruited from the
personnel at the Nestlé
Research Center.
Their heights ranged from 150 to 187 cm, and their weights ranged from 56 to 85
kg (body mass index range, 21.4 to 32.1 kg/m2). All subjects were
Caucasians. Exclusion criteria for enrollment were immunosuppression, gastric
problems, raised serum transaminase levels, antibiotic treatment during the
preceding 4 weeks, laxative use, pregnancy, and participation in other trials.
The protocol was approved by the local ethical committee, and the participants
provided written consent.
Study design.
The study was designed as a
single-center, randomized, and placebo-controlled study. The trial was a
double-blinded, three-period crossover comparison of two dosages of oral T4
phage conducted in June 2003 at our research center. Each subject received a
higher phage dose (dose A, with 105 PFU/ml), a lower phage dose
(dose B, with 103 PFU/ml), and placebo (dose C). The subjects were
randomly assigned to one of the following treatment sequences: ABC, BCA, and
CAB. The vehicle was 150 ml of mineral water (Vittel; pH 7.3; HCO3−,
258 mg/liter). For safety concerns, our medical advisor asked for the use of a
lower phage dose in our first human safety trial.
The study was divided into four
1-week intervals. The first week served as the baseline, during which two
random stool samples were taken. In the second week the subjects were
randomized and received 150 ml of the allotted mineral water three times per
day for 2 consecutive days (days 1 and 2), followed by 5 consecutive days
without the test mineral water (washout). This procedure was repeated for 3
consecutive weeks. During the study period the subjects provided all stool
samples produced each day. The code was broken only after the complete
acquisition of clinical and laboratory data. A clinical examination by a
physician was done at the start (day 0) and at the end (day 30) of the study,
and the volunteers received forms on which they could report any type of
adverse events.
Phage preparation.
Hershey medium was inoculated
with E. coli K803, a strain K-12 derivative lacking bacteriophage lambda
prophage, and was then infected with bacteriophage T4 (obtained from C.
Georgopoulos, Geneva University, Geneva,
Switzerland) at
37°C. The completely lysed culture was centrifuged at 4,000 × g for 15
min to remove bacterial debris. In parallel, mock-infected K803 was treated
with lysozyme and then sonicated. The supernatants were filtered through a
0.22-μm-pore-size Millipore filter. The phage was pelleted from the medium by
centrifugation (35,000 × g for 25 min), resuspended in 0.5 ml, and then
diluted to the desired titer with mineral water. Phage solutions were kept at
4°C, and no decrease in the phage titer was observed during the 1-month study
period in the plaque assay.
Polyacrylamide gel
electrophoresis, followed by silver staining, revealed in the resuspended T4
phage pellet no proteins which comigrated with proteins from the “phage”
preparation of the mock-infected K803 cell. Negative-staining electron
microscopy of the phage pellet showed a relatively pure phage fraction only
minimally contaminated with small cellular debris. In the Limulus test
(E-toxate kit; Sigma), 2 μg endotoxin/ml was detected in the phage pellet; 2 μg
carbohydrate/ml was measured as described by Dubois et al. (9).
No viable bacteria were detected in the phage preparation on Drigalski agar.
Laboratory evaluation.
Stools were stored at 4°C
immediately after defecation and were analyzed at the latest on the following
working day. We verified that phage titers did not decrease after overnight
storage. Five grams of each individual stool specimen was resuspended in 10 ml
of TS (8.5 g/liter NaCl, 1 g/liter tryptone), homogenized on a Vortex agitator,
and cleared by centrifugation at 4,000 × g for 15 min. One milliliter of
the supernatant was filtered through a Millex AP20 prefilter and through a
0.45-μm-pore-size Minisart filter. Fecal phage and E. coli were counted
as described previously (8).
T4-specific antibodies were tested by immunoglobulin G (IgG), IgM, and IgA
isotype-specific enzyme-linked immunosorbent assay (ELISA), performed as
described previously (4).
RESULTS
Safety.
All treatments were well
tolerated. Five mild adverse events were reported. Four were related to the
gut (stomach pain, nausea, increased peristalsis), and one volunteer reported
a sore throat. None of the gut-related events were severe enough to
necessitate treatment. Adverse events were not reported more often with the
higher phage dose than with the lower phage dose or placebo and were rated by
the study physician as unrelated to the study intervention.
Normal serum alanine
aminotransferase and aspartate aminotransferase levels were measured by an
accredited clinical laboratory before and after the study. No significant
increases in the levels of these two liver enzymes were observed. At the
beginning and at the end of the 1-month study period, the plasma samples from
all 15 volunteers were negative for T4 phage in the plaque assay (detection
limit, 10 PFU/ml), and no volunteer showed an increase in optical density by
the IgG-, IgM-, or IgA-specific ELISA with T4 phage coated on the plate (data
not shown).
Fecal phage excretion.
During the baseline
evaluation, none of the 15 volunteers excreted coliphage in their stool
samples, which could be detected on the K803 indicator. In contrast, 15 of 15
subjects showed fecal phage when they drank the mineral water with the higher
phage dose. We did not verify the identity of the orally ingested and fecally
excreted phage beyond its ability to grow on the indicator strain K803.
Thirteen of 15 subjects demonstrated at least one phage-positive stool sample
when they were exposed to the lower phage dose, while none of the volunteers
excreted phage when they were receiving the placebo (Fig. 1a
to e). The mean number of phage-positive stool samples differed
significantly between the two treatment groups: 4.4 and 1.3 positive stool
samples were observed for the 15 volunteers during the higher and lower phage
dose applications, respectively. Two subjects showed fecal phage only when
they received the high dose (Fig. 1f).
Figure 2a
presents the time course of phage prevalence in the stool samples for all
subjects. In both the group receiving the higher phage dose and the group
receiving the lower phage dose, all stool samples were phage negative on the
day before oral phage exposure. On the first day of phage exposure, less than
20% of the subjects were phage positive. On the second day of exposure to
oral phage, the prevalence increased to 80 and 50% for the higher and the
lower phage dose groups, respectively. In the group receiving the higher
phage dose, the stool phage prevalence rose to 100% on the third day, when
the volunteers were no longer receiving oral phage; remained at 90% on the following
day; and dropped only slowly over the next few days, with 38% phage-positive
stools 3 days after the cessation of oral phage application. A different type
of kinetics was seen in the group receiving the lower phage dose. A 50%
prevalence was still maintained on the day after phage exposure, but it then
dropped off very quickly. In both groups the oral phage took approximately 1
day to reach maximal prevalence in the feces. In the group receiving the
lower phage dose, the time for the washout of oral phage was again
approximately 1 day, reflecting a passive transit of the phage through the
gut.
Figure 2b
presents the mean fecal phage titers. The highest titers were found on the
second day after the subjects drank the mineral water with the higher phage
dose, but significant titers were still detected in the stools 1 day after
the subjects drank the last phage dose. Only very low mean fecal phage titers
were seen in volunteers receiving the lower phage dose; the peak mean titer
was 68; i.e., it was 500-fold lower than the peak mean titer in those
receiving the higher phage dose. The phage titers in the daily stool samples
describe a time profile. The area under the curve of this time profile is the
total amount of surviving T4 phage and was statistically analyzed as the
primary outcome. The difference between the groups receiving the higher and
the lower phage doses was statistically significant (P < 0.0001 in
a linear mixed model, P = 0.003 by the Kruskal-Wallis test).
Fecal E. coli count.
Each stool sample was
evaluated for its bacterial count on Drigalski agar. We determined previously
that the vast majority of the fecal colonies observed on this medium are E.
coli (8).
The E. coli counts for volunteers who were exposed to the sequence
placebo-higher phage dose-lower phage dose are shown in Fig. 1a
to e. There were substantial variations in these counts between subjects
and within the same subject. However, none of the subjects showed a
significant decrease in fecal E. coli counts that was associated in
time with application of the higher phage dose.
The fecal E. coli
counts in the daily stool samples describe a time profile. The area under the
curve of this time profile is the total amount of excreted fecal E. coli
and was statistically analyzed as the secondary outcome. The analysis was
performed by using a linear mixed-effect model (with Bonferroni's
correction). No differences were detected between the treatment and the
placebo groups (P > 0.99).
Random E. coli colonies
from the 15 volunteers were tested for their susceptibilities to phage T4
before and after the 3-week intervention period. Before the intervention, 12
of 168 colonies (7.1%) were susceptible to T4 phage, while after the
intervention only 1 of 116 colonies (0.9%) lysed in the presence of T4 phage.
|
DISCUSSION
One might question the use of
phage T4 in a safety trial for phage therapy since T4 has only a narrow host
range on E. coli. In fact, when T4 was tested for its lytic properties
on a collection of 42 E. coli strains representing 23 different somatic
O antigens, 10 different capsular K antigens, and 10 distinct H antigens (8),
only 2 strains were lysed in the cell tube test (S. Chibani-Chennoufi,
unpublished results). T4 is thus not a likely candidate for phage therapy but
was chosen as a surrogate for a first safety trial because it has been completely
sequenced and extensively characterized (12).
Recent genome analysis (16)
and 40 years of genetic research with T4 have not identified virulence genes on
its chromosome. In that respect, T4 differs clearly from lambda-like phages,
which frequently carry virulence genes (2,
3).
This difference between T4 and lambda phages is perhaps not surprising since T4
is the paradigm of an obligate lytic phage. Evolutionary reasoning suggests
that it is the coexistence of phage and bacterium in lysogeny which selects for
prophage genes that are of survival benefit to the bacterial host (5,
14).
In this small trial of oral
phage use, no significant adverse events were observed and the treatments were
well tolerated. Inchley (11)
showed that Kupffer cells of the liver phagocytized more than 99% of labeled T4
phage within 30 min after intravenous injection. The release of liver enzymes
should thus be a sensitive measure of liver toxicity from oral phages. However,
the serum levels of two liver transaminases did not increase with the
intervention. This observation is not so surprising, since with the low phage
doses used, no transit of the oral phage into the bloodstream was observed.
Mice fed a much higher oral dose of 1012 PFU of phage lambda showed
only between 10 and 1,000 PFU per ml of blood directly after exposure (10).
Within 10 h this phage was removed from the circulation. Likewise, phage lambda
injected into the bloodstream of mice was also quickly cleared in the spleen (10,
15).
However, clinical trials conducted in Eastern Europe
showed that oral phage enters the bloodstream (1,
18).
Yet, the absence of an anti-T4 immune response in our volunteers suggests that
no substantial amounts of T4 phage ever appeared in their circulation. The
ELISA protocol was sensitive enough to measure the serum antibody response 2
weeks after primary exposure of humans to oral rotavirus (4).
The fecal phage counts
demonstrated a dose-dependent appearance of the orally applied phage. While
they were on the “high” dose, the volunteers received a total of 9 × 107
PFU. Approximately 107 PFU phage was excreted into the stool, as
calculated from the mean fecal phage titers and the estimated stool volumes.
This value is strikingly close to the orally applied phage number, suggesting a
remarkable stability of the phage during gastrointestinal transit and only
small, if any, phage replication during the gut transit. This interpretation
concurs with the maintenance of the total fecal E. coli counts. However,
the possibility of destruction of the phage in the stomach, followed by
intestinal replication of the oral phage, cannot formally be excluded by the
current data. This interpretation is, however, less likely in view of previous
experiments with germfree mice (8).
It is clear that the present
study is only a first step in the assessment of the safety of oral phages.
Higher phage titers with a phage cocktail covering multiple E. coli
serotypes need to be tested. It will also be necessary to assess in more detail
the effect of phage on the composition of the commensal E. coli gut
microbiota.
Acknowledgments
We thank our colleagues at the
Nestle Research Center who served as volunteers, A. Blondel and S. Oguey-Araymon
for the daily care of the volunteers at our Metabolic Unit, J. Sidoti for
technical assistance, A. de Batz and D. Grathwohl for the statistical analysis,
A. Constable for critical reading of the report, and finally, Marianna Giarre
for the elaboration of the study master file.
REFERENCES
1.
Babalova, E. G., K. T. Katsitadze, L. A.
Sakvarelidze, N. S. Imnaishvili, T. G. Sharashidze, V. A. Badashvili, G. P.
Kiknadze, A. N. Meipariani, N. D. Gendzekhadze, E. V. Machavariani, K. L.
Gogoberidze, E. I. Gozalov, and N. G. Dekanosidze. 1968. Preventive value of dried dysentery
bacteriophage. Zh.
Mikrobiol. Epidemiol. Immunobiol. 45:143-145. (In Russian.).
2.
Boyd, E. F., and H. Brüssow. 2002. Common themes among bacteriophage-encoded
virulence factors and diversity among the bacteriophages involved. Trends Microbiol. 10:521-529. [PubMed]
3.
Brüssow, H., C. Canchaya, and W. D. Hardt. 2004. Phages and the evolution of bacterial pathogens:
from genomic rearrangements to lysogenic conversion. Microbiol. Mol. Biol. Rev. 68:560-602. [PubMed]
4.
Brüssow, H., H. Werchau, W. Liedtke, L. Lerner, C.
Mietens, J. Sidoti, and J. Sotek.
1988. Prevalence of antibodies to rotavirus in different age-groups of infants
in Bochum, West Germany. J. Infect. Dis. 157:1014-1022. [PubMed]
5.
Canchaya, C., C. Proux, G. Fournous, A. Bruttin, and
H. Brüssow. 2003. Prophage genomics. Microbiol. Mol. Biol. Rev. 67:238-276. [PubMed]
6.
Chibani-Chennoufi, S., C. Canchaya, A. Bruttin, and
H. Brüssow. 2004. Comparative genomics
of the T4-like Escherichia
coli phage JS98: implications for the
evolution of T4 phages. J. Bacteriol. 186:8276-8286. [PubMed]
7.
Chibani-Chennoufi, S., J. Sidoti, A. Bruttin, M. L.
Dillmann, E. Kutter, F. Qadri, S. A. Sarker, and H. Brüssow. 2004. Isolation of Escherichia coli bacteriophages from the stool of pediatric diarrhea
patients in Bangladesh.
J. Bacteriol. 186:8287-8294. [PubMed]
8.
Chibani-Chennoufi, S., J. Sidoti, A. Bruttin, E.
Kutter, S. Sarker, and H. Brüssow.
2004. In vitro and in vivo bacteriolytic activities of Escherichia coli phages: implications for phage therapy. Antimicrob. Agents Chemother. 48:2558-2569. [PubMed]
9.
Dubois, M., K. A. Gilles, J. K. Hamilton, P. A.
Rebers, and F. Smith. 1956.
Colorimetric method for determination of sugars and related substances. Anal. Chem. 28:350-356.
10.
Geier, M. R., M. E. Trigg, and C. R. Merril. 1973. Fate of bacteriophage lambda in non-immune
germ-free mice. Nature 246:221-223. [PubMed]
11.
Inchley, C. J. 1969. The activity of mouse Kupffer cells following intravenous
injection of T4 bacteriophage. Clin. Exp. Immunol. 5:173-187. [PubMed]
12.
Karam, J. D.
1994. Molecular biology of bacteriophage T4. ASM Press, Washington, D.C.
13.
Kutter, E., and A. Sulakvelidze. 2005. Bacteriophages: biology and applications. CRC
Press, Inc., Boca Raton, Fla.
14.
Lawrence, J. G., R. W. Hendrix, and S. Casjens. 2001. Where are the pseudogenes in bacterial genomes? Trends Microbiol. 9:535-540. [PubMed]
15.
Merril, C. R., B. Biswas, R. Carlton, N. C. Jensen,
G. J. Creed, S. Zullo, and S. Adhya.
1996. Long-circulating bacteriophage as antibacterial agents. Proc. Natl. Acad. Sci. USA 93:3188-3192. [PubMed]
16.
Miller, E. S., E. Kutter, G. Mosig, F. Arisaka, T. Kunisawa,
and W. Ruger. 2003. Bacteriophage T4
genome. Microbiol.
Mol. Biol. Rev. 67:86-156. [PubMed]
17.
Sulakvelidze, A., Z. Alavidze, and J. G. Morris, Jr. 2001. Bacteriophage therapy. Antimicrob. Agents Chemother. 45:649-659. [PubMed]
18.
Weber-Dabrowska, B., M. Dabrowski, and S. Slopek. 1987. Studies on bacteriophage penetration in patients
subjected to phage therapy. Arch. Immunol. Ther. Exp. (Warsaw) 35:563-568.
Articles from Antimicrobial
Agents and Chemotherapy
are provided here courtesy of
American Society for Microbiology (ASM)
American Society for Microbiology (ASM)
Figure 2
Figure 1
Antimicrob
Agents Chemother. 2005 July; 49(7): 2874–2878.
doi:
10.1128/AAC.49.7.2874-2878.2005.
|
PMCID: PMC1168693
|
..............................................
Anthrax stopper
Travis, John
Science News
08-24-2002
SCIENCE NEWSThis Week
Viral enzyme detects, kills bacterium
Last fall, envelopes full of anthrax-causing spores killed 5 people, sickened about a dozen, and struck fear in millions. Researchers funded by the U.S. military have now developed an innovative way to detect and kill Bacillus anthracis, the bacterium that causes anthrax. Seeking help from nature, the researchers are using an enzyme produced by a bacteriophage, a virus that preys upon bacteria.
The enzyme, called lysin, prevented the death of most mice that the researchers had infected with a bacterial relative of B. anthracis, Raymond Schuch of Rockefeller University in New York and his colleagues there report in the Aug. 22 Nature. The investigators also used the enzyme to create a prototype handheld instrument that quickly detects the anthrax bacterium, even in its spore form.
"This is avery clever exploitation" of lysin, says biowarfare researcher Stephen Morse of Columbia University.
Bacteriophages, or phages, infect bacteria in order to reproduce inside. Once they do, phages use lysin to break apart their hosts cell walls so the new phages can infect other bacteria "They cause the [bacterium] to explode," says study coauthor Vincent A. Fischetti.
Discovered nearly a century ago, bacteriophages have long attracted the interest of physicians seeking to control bacterial infections. Antibiotics stole the spotlight from phage therapy for many decades, but there's renewed interest in the strategy, given the rise of antibiotic-resistant bacteria (SN: 6/1/96, p. 350; 6/3/00, p. 358).
Over the past few years, Fischetti and his colleagues have exploited the bacteria-- killing talent of phages in a different way. They've shown that lysin itself represents a new way to destroy bacteria. For example, they've successfully used lysin to treat animals infected with bacteria that cause strep throat and pneumonia in people (SN: 6/10/00, p. 376).
Fischetti's group recently turned its attention to potential biowarfare agents, starting with the anthrax bacterium. While conventional antibiotics can treat many strains of B. anthracis, there's concern that resistant strains could evolve or be created, says Fischetti.
He and his colleagues began working with a phage that infects the anthrax bacterium almost exclusively and identified the gene encoding its lysin. In test-tube experiments, the enzyme destroyed strains ofB. anthracis collected from around the world but left most other bacteria unscathed.
Next, the scientists tested the enzyme on mice infected with a strain of Bacillus cereus closely related to the anthrax bacterium. This strain serves as an initial testing ground for anthrax therapies because B. anthracis is so dangerous to work with. The B. cereus strain typically kills infected mice, but treatment with lysin saved up to 76 percent of infected animals, Fischetti's team reports.
The researchers now plan to test the enzyme against B. anthracis, first in rodents and then in a nonhuman primate. If those experiments prove successfull, physicians would then assess the safety of the viral protein in human volunteers. If lysin passes muster, the U.S. and other governments could then consider stockpiling the enzyme for any future anthrax attack
Fischetti's group also built a B. anthracis detector. The investigators mixed lysin with chemicals that emit a flash of light when exposed to a substance released by dead bacteria. They also added an agent that induces B. anthracis spores to germinate, making them susceptible to lysin. Finally, they engineered a handheld light meter to monitor this broth and found it could detect a signal produced by as few as 100 spores within an hour of adding them to the broth.
"It's an innovative and promising strategy," says Morse.
Copyright Science Service, Incorporated Aug
24, 2002
Commercial Companies Involved in Phage R @ D
Biochimpharm
Contact Information:
Alexandr Golejashvili, Tbilisi, Georgia
Montreal, Canada
Phone: (514) 496-1488
Fax: (514) 496-1521
Email: email@biophage.com
Dr. Goda Krishna
#5 AC, 705 II Block, Hennur Road
Banaswadi Layout, Bangalore 560043
Phone: +91-80-5448138/5448146
Fax: 91-80-5447996
Email: godakrishna@gangagen.com
Biochimpharm owns the large privatized production facility for phage tablets and
some other products in the main building. The company was only formed in
2000 and is licensed to produce dysentary tablets and several other
products, but has been able to make only limited use to date of the
large facilities. The area is in relatively good shape physically, with
large if old fermenters and excellent filtration devices and machines
that could make 100,000 tablets per hour. They have just been awarded an
ISTC grant in combination with the Eliava Institute's Liana
Gachechiladze to focus on Serratia as well as Pseudomonas. They are
negotiating the final work plan and beginning some refurbishing
Contact Information:
Rosemonde Mandeville
Montreal, Canada
Phone: (514) 496-1488
Fax: (514) 496-1521
Email: email@biophage.com
…………………………………………………………………………………………………………………………………………………………
Biopharm Pharmaceuticals
Contact Information:
Lado Gulisashvili and Lela Kalandarishvili
Tbilisi, Georgia
Email: biopharm@got.ge
Tbilisi, Georgia
Email: biopharm@got.ge
Biopharm
obtained most of original big main production plant of the Eliava
Institute after privatization, and has enhanced its capacity with much
good equipment obtained from bankrupt companies, including in Moscow.
They make vitamins, various biomedical reagents, probiotics, and
currently also about 20 liters a month of phage products, including
pills. They use primarily the phages that were being produced before
privatization, with some research focused on methods of delivery that
can be patented, such as new capsule formulations
………………………………………………………………………………………………………………………………………………………………
Contact Information:
Richard Carlton, M.D.
150 Main Street
Port Washington, NY 11050
Phone: (516) 883-6883
Fax: (516) 883-6903
Email: carltonebi@erols.com
150 Main Street
Port Washington, NY 11050
Phone: (516) 883-6883
Fax: (516) 883-6903
Email: carltonebi@erols.com
……………………………………………………………………………
Contact Information:
J. Ramachandran
3279 Emerson
Palo Alto, CA 94306
Phone: 650-856 9118
Fax: 650-856 9642
Email: jram@gangagen.com
3279 Emerson
Palo Alto, CA 94306
Phone: 650-856 9118
Fax: 650-856 9642
Email: jram@gangagen.com
Gangagen Life Sciences Inc:
Dr. Kishore Murthy,
Chief Scientific Officer
1740, Woodroffe Ave,
Building 400, Suite # 2
Ottawa, Ontario, K2G3R8
Email: kmurthy@gangagen.com
Dr. Kishore Murthy,
Chief Scientific Officer
1740, Woodroffe Ave,
Building 400, Suite # 2
Ottawa, Ontario, K2G3R8
Email: kmurthy@gangagen.com
Gangagen Biotechnologies Ltd:
Dr. Goda Krishna
#5 AC, 705 II Block, Hennur Road
Banaswadi Layout, Bangalore 560043
Phone: +91-80-5448138/5448146
Fax: 91-80-5447996
Email: godakrishna@gangagen.com
Contact Information:
HEXAL Gentech ForschungsGmbH
Industriestr. 25, 83607
Holzkirchen, Germany
Email: info@greinerbioone.com
Industriestr. 25, 83607
Holzkirchen, Germany
Email: info@greinerbioone.com
Immunopreparat Research Productive
Association
Contact Information
:
Novorossiiskaya 105, 450024
Ufa Bashkortostan, Russian Federation
Ufa Bashkortostan, Russian Federation
Immunopreparat
is a large pharmaceutical company in Russia, which is located
in the
city of Ufa (approximately 60 miles west of the Ural Mountains). The company’s subsidiary, Biophag, currently manufactures at least two
complex phagepreparations (“Bacteriophagum” and “Piobacteriaphagum”) targeting various bacterial pathogens
………………………………………………………………………………………………………………………………………………………………………………
Contact Information:
Contact: Torrey Brown
The Warehouse at Camden Yards
323 W. Camden Street, Suite 675
Baltimore, Maryland 21201
Phone: (410) 659-7330
Fax: (410) 625-2323
EMail: info@Intralytix.com
The Warehouse at Camden Yards
323 W. Camden Street, Suite 675
Baltimore, Maryland 21201
Phone: (410) 659-7330
Fax: (410) 625-2323
EMail: info@Intralytix.com
………………………………………………………………………………………………………………………………………………………………………………..
Micropeace
Contact Information:
Contact: Dr. Ipek Kurtboke
LPO Box 2093
Hawthorn, Melbourne, Victoria 3122
Australia
Phone: +61 (03) 9813 5660
Fax: +61 (03) 9813 5660
Email: micropeace@hotmail.com
LPO Box 2093
Hawthorn, Melbourne, Victoria 3122
Australia
Phone: +61 (03) 9813 5660
Fax: +61 (03) 9813 5660
Email: micropeace@hotmail.com
Developing
new compounds for future use against drug-resistant bacteria and/or for
chemical modifications for field applications by screening for new
metabolites and evaluating the potential of less known or new bacteria
taxa.. Bacteriophage are being used as natural indicators of the
presence of rare taxa in a selected test substrate, to determine the
relatedness of the isolated taxa and to deselect unwanted taxa on
isolation plates in the process of target specific selective isolation.
Micropeace provides consultancy to biotechnology companies and research
institutes interested in detection of rare or novel actinomycetes and
other bacteria on ways to use phages as effective tools in this search.
…………………………………………………………………………………………………………………………………………………………………………………..
Contact Information:
Dr J. Nick Housby, PhD – Chief Executive Officer and Director
j.n.housby@novolytics.co.uk
Professor Nick H Mann, PhD – Chief Scientific Officer and Director
n.mann@novolytics.co.uk
Warwick Ventures
University House
Kirby Corner Road
Coventry, UK CV4 8UW
j.n.housby@novolytics.co.uk
Professor Nick H Mann, PhD – Chief Scientific Officer and Director
n.mann@novolytics.co.uk
Warwick Ventures
University House
Kirby Corner Road
Coventry, UK CV4 8UW
Contact Information:
Asher Wilf
4, Pekeris St., Rabin Science Park
Rehovot 76702, Israel
Cell: +972-52-446782
Phone: 972-8-947-1837
Fax: +972 8-947-1845
Email: asher@phage-biotech.com or info@phage-biotech.com
4, Pekeris St., Rabin Science Park
Rehovot 76702, Israel
Cell: +972-52-446782
Phone: 972-8-947-1837
Fax: +972 8-947-1845
Email: asher@phage-biotech.com or info@phage-biotech.com
Contact Information
Dr Anthony M. Smithyman, Managing Director
7/27 Dale Street
Brookvale
NSW 2100 Australia
Smithyman@cellabs.com.au
phone: +61 2 9905 0133
fax: +61 2 9905 6426
7/27 Dale Street
Brookvale
NSW 2100 Australia
Smithyman@cellabs.com.au
phone: +61 2 9905 0133
fax: +61 2 9905 6426
Special
Phage Services Pty Ltd. was established in October 2002 as a specialist
phage therapy services company by immunologist Dr. Anthony Smithyman.
SPS is a start-up company formed in response to the growing concern of
antibiotic resistance and the need for alternative solutions to
antibiotic use. SPS has access to phage production know-how as well as a
phage library of over 3,000 strains through an exclusive license with a
well known Georgian-based company. SPS plans to develop and
commercialise in Australasia and Asia a range of proprietary, tailored
phage therapeutics (SmartPhageTM) for use in human and animal health,
food and environmental markets.
Contact Information
7170 Frederick Banting
2nd Floor
St. Laurent, QC H4S 2A1
phone: (514) 332-1008
fax: (514) 332-6033
2nd Floor
St. Laurent, QC H4S 2A1
phone: (514) 332-1008
fax: (514) 332-6033
Targanta
is developing small-molecule antibacterial agents aiming at the
disruption of the DNA replication and transcription machinery through
the targets of bacteriophages (“phages”), viruses that attack bacteria.
This approach effectively mimics strategies devised through four billion
years of evolutionary pressure with regards to the selection of
druggable bacterial targets, in contrast to current drug discovery
efforts, which often focus on comparative functional bacterial genomics.
The Company has been able to identify the molecular interactions
enabling phages to hamper bacterial sustainability, and thereby has
validated an innovative process for identifying novel drug targets and a
new class of proprietary antibacterial molecules. Targanta's approach
circumvents the demonstrated limitations of sequencing bacterial genomes
as a way to identify novel antibacterial targets and new classes of
antibacterials. The Company is in the process of converting this unique
expertise in terms of target validation into novel antibacterial drugs
Biochimpharm
owns the large privatized production facility for phage tablets and
some other products in the main building. The company was only formed in
2000 and is licensed to produce dysentary tablets and several other
products, but has been able to make only limited use to date of the
large facilities. The area is in relatively good shape physically, with
large if old fermenters and excellent filtration devices and machines
that could make 100,000 tablets per hour. They have just been awarded an
ISTC grant in combination with the Eliava Institute's Liana
Gachechiladze to focus on Serratia as well as Pseudomonas. They are
negotiating the final work plan and beginning some refurbishing
THE NEXT PHAGE
Popular Science April 2009
By Elizabeth Svoboda Posted 03.31.2009 at 7:11 am
How to heal an infection that defies antibiotics? Another infection. Doctors in Eastern Europe have used lab-grown viruses to safely cure millions of wounds. So why can't we do the same here?
It seemed like nothing at first. The red patch that appeared on Roy Brillon's thigh could have been a spider bite. But as the weeks passed, it grew and grew. By December 2004, the innocuous-looking bump had become an open wound the size of the palm of his hand. Brillon's doctor, Randy Wolcott, prescribed just about every antibiotic he could think of to cure the infection, but the lesion just got worse. "It was really bad," says Brillon, a 62-year-old retired housepainter from Lubbock, Texas. "I had to give up work because I couldn't climb ladders anymore."
Brillon felt like he was being eaten away from the inside out. And in a very real sense, he was. Left unchecked, bacteria like the streptococcus and staphylococcus devour soft tissue to keep themselves alive, leaving ragged red edges that expand outward with terrifying aggression. The pain in his leg was so excruciating that Wolcott prescribed morphine. "I was only supposed to take two pills a day, but I was taking three in the morning and three in the afternoon," he says. "The pain is indescribable. You just grit your teeth."
As head of Lubbock's Southwest Regional Wound Care Center, Wolcott knew well the typical prognosis for patients with antibiotic-resistant infections like Brillon's: gangrene, amputation and, for about 100,000 Americans a year, death. " 'Chronic wound' is a code word for 'you can't heal it,' " he says. "The hallmark is, we cut it off or we cut it out. It's pretty barbaric." Wolcott was desperate for an alternative. After putting in 10-hour days at the clinic, he often sat up late at night poring over medical journals for the newest wound-care research—something, anything that might help patients with the most intractable infections.
When Brillon arrived for a follow-up appointment three weeks later, Wolcott entered the room with a dropper in one hand and a vial of liquid that looked suspiciously like pond water in the other. The liquid, it turned out, was Wolcott's "anything": a murky concoction filled with bacteria-eating viruses known as bacteriophages. Physicians in Eastern Europe, Wolcott had explained to Brillon earlier, have been using phages safely since the 1920s to treat conditions that defy conventional antibiotics, from strep and tuberculosis to infected sores like his. Even U.S. drug companies sold them until the early 1940s, when penicillin came along and proved easier to use, generally more effective and, in the end, more lucrative than phages. The viruses might not help, he admitted, but if they didn't hurt, what was the harm in trying?
Brillon didn't need much convincing. The Food and Drug Administration was another story. Since 1963, the agency has mandated a strict approval process for all medications sold in America. Phage therapy has yet to be subjected to it, so Wolcott had to petition his state regulatory board to allow him to administer it only to people who had exhausted all other options. Then, because you can't find phages in U.S. pharmacies, he had to trek all the way to the former Soviet republic of Georgia to get it. There it's sold over the counter like eyedrops. He bought, for $2 each, three clear glass bottles, each filled with a liquid containing hundreds of types of phages.
"That's it?" Brillon asked, after Wolcott dribbled a few drops of the yellowish liquid onto his wound. The stuff was painless. Nothing much happened over the first few days, and Brillon braced himself for another disappointment. But as the week passed, the sore began to fade to a healthier pink, and then a new island of healthy skin emerged, expanding steadily every day. Within three weeks, the wound was completely healed. "You'd better take pictures of this," Brillon told Wolcott, "or nobody is going to believe it."
BRILLON'S RECOVERY was astonishing, but it wasn't a one-shot deal. Wolcott had also given the phage solution to 10 of his other worst-case patients, and many of them were showing similar results. If phages worked for them, Wolcott reasoned, couldn't they also work for the millions of patients in the U.S. living with infections resistant to antibiotics? His patients, he felt, were proof of it. The real question was whether he could convince the FDA.
As viruses go, phages are relatively benign. They're the most abundant naturally occurring organisms on Earth. They can be found virtually everywhere-in soil, drinking water, sewage. In fact, each one of us naturally has billions of them in our bodies. They prey only on bacteria, never human cells, they rarely spread from person to person, and, perhaps most important, bacteria have trouble becoming immune to them. As living organisms, phages are constantly changing and adapting in tandem with their host bacteria to kill them more effectively. Phage therapy could therefore eliminate the vicious cycle in which bacteria evolve resistance to antibiotics, necessitating the development of new, even more powerful drugs, at which point the process begins all over again.
But there's a big sticking point. The very characteristic that makes phages so effective-that expert ability to shape-shift- makes it difficult for them to pass muster with U.S. regulatory authorities. Although there have been no reports of adverse effects resulting from mutations, phages that don't normally nest inside the human body could potentially swap genes with other phages that do and produce foreign proteins that trigger an immune reaction. And it's impossible to say exactly how a virus might mutate when exposed to different bacteria, says Paul Sullam, a microbiologist at the University of California at San Francisco. For that reason, among others, says FDA spokesperson Karen Riley, phage therapy used to treat or cure humans must be regulated as a biological product. That means that if the viruses show serious signs of mutating or changing during clinical trials, even if those changes pose no risk to patients, the trials could be scrapped. Which explains why Big Pharma isn't eager to conduct them. "I understand where the FDA is coming from, because each phage poses a certain risk," Sullam says. "When viruses have the ability to exchange genetic material, it makes people nervous on a visceral level."
TO THE FDA, the serum Randy Wolcott drizzled on his patient's leg is new and unproven. But to the scientists working at the George Eliava Institute of Bacteriophage, Microbiology and Virology in the republic of Georgia, the medicine is as trusted as aspirin. Since 1923, when the facility was founded, scientists there have successfully treated millions of patients with phage therapy and presented more than 100 research abstracts at international conferences attesting to its clinical value.
Wolcott calls Eliava the "mother ship of phage research," a worldwide Mecca for people suffering from antibioticresistant infections. Only it doesn't look like the sort of place you'd want to go with a health problem. When Wolcott visited to hunt down alternatives for his patients, the four-story facility bore a closer resemblance to a neglected sanatorium. The walls were unpainted, the rooms were dark, and the equipment looked like museum pieces. "The conditions were abysmal," he says. "Yet the science is amazing."
Wolcott spent five days shadowing the staff and learning about phage therapy firsthand. "They had these 10-foot-tall fermenters, like big cooking pots, and they used them to make millions of doses of phage medication a year," he says. What surprised him most, aside from the dreary decor, was the painstaking way each prescription was custom-tailored for the patient. Phages are species-specific-different strains attack different bacteria. Since some wounds can harbor hundreds of different types of bacteria, physicians there first culture a tissue sample of the infection to determine its precise bacterial composition. The next step is to brew a custom cocktail of sometimes hundreds of phages selected from the institute's vast library of thousands. This whole process can take up to four days. The treatment-often administered through an IV bag that drips phage liquid directly into patients' wounds for 24 hours a day-can last up to two weeks.
As inconvenient as the procedure sounds, few people complain about it. The results are spectacular, Wolcott says: "I met a woman with a chronic ear infection who was coming back to the phage clinic for her final appointment. They gave her the therapy, and within a week, she was completely cleared up." In fact, studies published over the past several decades, based on trials conducted at Eliava and elsewhere in Eastern Europe, have shown that phage therapy has an 80 to 90 percent success rate against bacteria likely to show antibiotic resistance, such as Staphylococcus aureus and Escherichia coli. In contrast, many antibiotics fail outright against the evolved forms of these pathogens. In June 2005, a bacterial strain resistant to the first-line antibiotic imipenem ravaged more than 50 patients at New York City hospitals. Among patients whose infections infiltrated their bloodstream, the death rate was 47 percent.
With antibiotic resistance reaching record levels worldwide, phage therapy is no longer the sole province of Eastern European researchers. British biotech firm Biocontrol wrapped up the first Phase II clinical trial of phages in Western Europe last year with dramatic results. Its phage regimen combats the Pseudomonas aeruginosa bacterium, which causes serious lung and ear infections and is highly resistant to antibiotics. Patients with antibiotic-resistant infections who received phage therapy experienced a 50 percent reduction in their symptoms, compared with only a 20 percent decrease in the group that did not receive phages. "Frankly, I was blown away," says Dan Nelson, a biochemist at the University of Maryland who was at the conference where Biocontrol unveiled its results.
For Wolcott, who watches hundreds of patients die every year from seemingly incurable infections, these medicinal viruses can't arrive in the U.S. fast enough. "Phage needs to be fast-tracked. It works. It's completely natural. Why can't you spray this stuff on a kid's throat right now?"
IN TRUTH, phage therapy is already here, just not in a way that's practical for Wolcott. Owing to a regulatory technicality, manufacturers can use phages to keep ready-to-eat foods like deli meat and coleslaw safe from bacterial contamination, but doctors can't prescribe them to treat a bad case of strep. The difference, according to the FDA, is the application: Spraying a phage on lunch meat makes it a food additive. Give it to someone with an infection, and it becomes a drug. In 2006, the biotechnology company Intralytix took advantage of the less stringent regulatory rules for food additives to secure FDA clearance to sell a phage spray that kills Listeria bacteria, a common source of food poisoning. The company is also developing several phage treatments for humans, one of which entered clinical trials, thanks to Wolcott.
Wolcott met Intralytix CEO John Vazzana at a phage conference in Texas three months after he returned from Europe. The two talked for hours about the frustrating plight of phages in the U.S. By the end of the conference, they had hatched a plan to convince the FDA to let them start a clinical trial. Intralytix would supply the phages; Wolcott, the patients.
The FDA eventually agreed, on the condition that they limit the trial to only eight well-studied Intralytix phage strains. Wolcott quickly recruited 39 patients, all with infected venous leg ulcers, and set about conducting a two-year trial, the first of its kind on this side of the Atlantic.
Every week, Wolcott's study participants arrived at the clinic and received their phages through a handheld ultrasonic device, a high-tech upgrade to the IV drips common in Eastern Europe. The device simultaneously sprays on saline-based phage solution and destroys blackened or dead tissue, allowing the phages to penetrate deeper into the wound. Like all initial clinical trials, Wolcott's was designed to assess the safety of the therapy, not its outright effectiveness. In this context, the study yielded promising signs for the future. None of the patients in the trial reported severe side effects, but the efficacy was unimpressive. Nearly 70 percent of the volunteers experienced significant healing by the end of the 24-week trial period, as did a similar percentage of trial patients who did not receive the phage. Wolcott anticipated this, and attributes it to the fact that the cocktail was not tailored to combat the particular bacteria in his patients' wounds, as is standard practice in Georgia, limiting the phages' potency.
And this is where Wolcott hits a wall. FDA regulators have told him that if he wants to use phages on his patients, he's going to have to carry out a separate clinical trial for each phage or particular mix of phages he hopes to administer, just as he would if he were shepherding distinct chemical compounds through the regulatory process. But since each of his patients' wounds might contain hundreds of different species of bacteria, he can't reasonably attempt to conduct trials of the thousands of phage combinations required to combat them all, especially considering that the cost of a trial for a single drug can easily run into the millions. "People in this country have a right to be incensed that we have a very different situation here than in Europe with regards to phage," says Betty Kutter, a phage researcher at Evergreen State College. "Our whole regulatory environment has been one major thing that has slowed people down."
A Phase II efficacy trial enrolling 100 to 200 wound patients would cost about $9 million-and if the therapy being tested included only a few types of phages, as the first trial did, there's a good chance it wouldn't pan out for patients whose infections are caused by multiple strains of bacteria. And given the current regulations, Vazzana isn't sure he could even find the capital to fund the trial.
But phage researchers like Ben Burrowes of the Texas Tech University Health Sciences Center are optimistic. "Companies will start coming out with phage products at some point," he says, "and once those first few get through the approval process, the FDA will relax its standards a little."
RockefelleR university biologist Vincent Fischetti, for one, isn't holding his breath. Fischetti has no doubt that there's a gaping hole in the health-care landscape where effective antibacterial drugs should be. He just isn't sure phages are the best way to fill the void. To him, Wolcott and his fellow phage-therapy practitioners are like peacekeepers with no governmental backing: wellintentioned, to be sure, but unlikely to have much success in the end. "I'm not working on phage therapy," he insists, as he guides me through his sixth-floor lab overlooking the institute's Manhattan campus. "I'm working on phage-based therapy."
This distinction might seem arcane to nonbiologists, but in Fischetti's mind, it's a crucial one. While Wolcott sees phages as a major therapeutic coup, Fischetti sees them as merely an intermediate step toward a new generation of even better bacteria-fighters. He contends that the uphill regulatory battle phages face, as well as the risk of mutations, make them too big a gamble for American drug companies. "Phages are going to be a boutique treatment, nothing more," he says.
So he is taking an alternative approach, purifying the phage to extract the lysin, the enzyme it uses to dissolve the bacterial cell wall and kill the bacterium. He enlists his lab staff to serve as biological prospectors, collecting the bacteria-killing viruses from swamps, rivers, anywhere they can find them. He points to a bag of smelly bat excrement on his windowsill. "We can take the phages out of that stuff."
Having observed that lysins were the phages' "active ingredients," Fischetti aims to harvest the lysins from them and turn them into stable antibacterial drugs. If successful, he could accomplish a double feat previously thought impossible: getting the bacteria-fighting benefits of phages to patients, while doing an end run around the regulatory Rube Goldberg machine that researchers like Wolcott face.
Whereas phages must evolve to keep up with bacterial evolution, lysins are like a blunt instrument that can kill entire families of bacteria, eliminating the need to isolate and test thousands of different compounds as phage scientists in Georgia do. But even if the FDA might perceive lysins more favorably than phages alone, Kutter says, the enzymes have drawbacks of their own. Lysins work only on Gram-positive bacteria, like strep and staph, not Gram-negative bacteria like E. coli and salmonella-the Gram-negative bacteria have an outside membrane that the lysins can't get through. Phages, on the other hand, can work against both kinds of bacteria. And unlike traditional phage therapy, lytic enzymes haven't made it to clinical trials yet, so although petri-dish evidence is promising, there's no telling whether it will translate into success in a hospital setting.
It's clear that unless the FDA is willing to consider revised approval guidelines, phage therapy in the U.S. will remain in a holding pattern indefinitely. And in Lubbock, Roy Brillon's life has settled into a similar stasis. The phage Wolcott brought back from Georgia healed his leg wound, but since Brillon has problems with the valves that control blood flow in his leg veins, he's constantly developing new sores. "The blood goes down the veins, but it can't go back up," he explains. "The sores shrink and then pop up somewhere else on my leg."
What Brillon really needs, Wolcott says, is a phage cocktail custom-mixed to target the particular bacteria colonizing his wounds. But it's back to the same old antibiotics for now. Sometimes, if the bacteria happen to be non-drug-resistant, the antibiotics work; sometimes they yield about the same results as a newt's-eye potion. Brillon keeps his legs wrapped in Ace bandages like a burn victim. "If you don't keep 'em tight," he says, "then the legs swell, and that's when the sores come out."
But he's not dwelling on the obstacles. Instead he imagines the day when he'll be able to put his infections behind him for good and spend more time fishing and playing with his four grandchildren who live nearby. He figures that if anyone can get him there, it will be Wolcott and his army of phages. "It really bothers him if he gets ahold of something he can't handle," Brillon says. "He tells me, 'I'm never going to give up on you.' "
Elizabeth Svoboda is a contributing editor at Popular Science. Her last feature article, in July 2007, was about research efforts to turn algae into clean-burning biodiesel.
Copyright Bonnier Corporation Apr 2009
........................................................
Cholesterol-lowering statins boost bacteria-killing cells
Posted On: November 17, 2010 - 5:40pm
Cholesterol-lowering statins boost bacteria-killing cells
Posted On: November 17, 2010 - 5:40pm
Science Codex
Widely prescribed for their cholesterol-lowering properties, recent
clinical research indicates that statins can produce a second,
significant health benefit: lowering the risk of severe bacterial
infections such as pneumonia and sepsis. A new explanation for these
findings has been discovered by researchers at the University of
California, San Diego School of Medicine and Skaggs School of Pharmacy
& Pharmaceutical Sciences, who describe for the first time how
statins activate the bacterial killing properties of white blood cells.
The research is published in the November 18, 2010 issue of Cell Host & Microbe.
Led by Victor Nizet, MD, professor of pediatrics and pharmacy, and Christopher Glass, MD, PhD, professor of medicine and cellular & molecular medicine, the UC San Diego team found that phagocytes (white blood cells that kill and ingest harmful bacteria, foreign particles and dead or dying cells) became more effective after being exposed to statins.
Surprisingly, the statin-induced improvement in bacterial killing did not correspond to increased uptake of bacteria by these specialized white blood cells. Rather, the researchers found that statins stimulated the phagocytes to release "extracellular traps" – specialized webs of DNA-based filaments embedded with anti-microbial peptides and enzymes capable of ensnaring and killing bacteria before they spread in the body.
The findings have broad ramifications, said Glass, given the popularity of statins for controlling high cholesterol levels. Statins are the world's most-prescribed class of medication. An estimated 30 million Americans alone take the drug under commercial names like Lipitor, Zocor and Crestor. "Clinical research indicates that perhaps 100 million Americans have elevated cholesterol levels that could benefit from statin therapy," said Glass. "Thus any statin-associated changes to immune system function are certain to impact millions of people."
Prior research had described various anti-inflammatory properties of statins, suggesting that these effects could contribute to a reduction in disease severity during severe infections. Nizet and Glass explored a different hypothesis: That statins might actually aid the body in clearing itself of infectious microbes. The researchers focused on Staphyloccocus aureus, more commonly called "staph," a frequently antibiotic-resistant human pathogen responsible for everything from minor skin infections to life-threatening meningitis and sepsis. Mice treated with statins were more resistant to staph infections, and phagocytes isolated from these mice were more effective at killing staph bacteria. Simple exposure of freshly isolated human white blood cells to statins in a test tube markedly increased their ability to kill staph and other important disease causing bacteria. In each case, the increased killing correlated with greater release of the DNA-based extracellular traps by the phagocytes.
The UCSD findings demonstrate that statins have important pharmacological effects beyond inhibiting cholesterol production. "We found these drugs fundamentally alter how white blood cells behave upon encountering bacteria," Nizet said. "In our studies with staph bacteria, the net effect of statin treatment was to improve bacterial killing and extracellular trap formation. These same changes might not be so consequential for defense against less virulent bacteria that are easily susceptible to uptake and killing within phagocytes."
The research also sheds important new light on the clinical phenomenon of reduced infection severity in patients receiving statins, the scientists said. It indicates that levels of cholesterol or related lipid molecules can be sensed by white blood cells and used as signals to control their inflammatory and antibacterial activities. Nizet and Glass recommend that future research explore whether the potential of cholesterol-lowering agents combined with antibiotics can be harnessed to optimize the treatment of certain difficult infectious disease conditions.

The research is published in the November 18, 2010 issue of Cell Host & Microbe.
Led by Victor Nizet, MD, professor of pediatrics and pharmacy, and Christopher Glass, MD, PhD, professor of medicine and cellular & molecular medicine, the UC San Diego team found that phagocytes (white blood cells that kill and ingest harmful bacteria, foreign particles and dead or dying cells) became more effective after being exposed to statins.
Surprisingly, the statin-induced improvement in bacterial killing did not correspond to increased uptake of bacteria by these specialized white blood cells. Rather, the researchers found that statins stimulated the phagocytes to release "extracellular traps" – specialized webs of DNA-based filaments embedded with anti-microbial peptides and enzymes capable of ensnaring and killing bacteria before they spread in the body.
The findings have broad ramifications, said Glass, given the popularity of statins for controlling high cholesterol levels. Statins are the world's most-prescribed class of medication. An estimated 30 million Americans alone take the drug under commercial names like Lipitor, Zocor and Crestor. "Clinical research indicates that perhaps 100 million Americans have elevated cholesterol levels that could benefit from statin therapy," said Glass. "Thus any statin-associated changes to immune system function are certain to impact millions of people."
Prior research had described various anti-inflammatory properties of statins, suggesting that these effects could contribute to a reduction in disease severity during severe infections. Nizet and Glass explored a different hypothesis: That statins might actually aid the body in clearing itself of infectious microbes. The researchers focused on Staphyloccocus aureus, more commonly called "staph," a frequently antibiotic-resistant human pathogen responsible for everything from minor skin infections to life-threatening meningitis and sepsis. Mice treated with statins were more resistant to staph infections, and phagocytes isolated from these mice were more effective at killing staph bacteria. Simple exposure of freshly isolated human white blood cells to statins in a test tube markedly increased their ability to kill staph and other important disease causing bacteria. In each case, the increased killing correlated with greater release of the DNA-based extracellular traps by the phagocytes.
The UCSD findings demonstrate that statins have important pharmacological effects beyond inhibiting cholesterol production. "We found these drugs fundamentally alter how white blood cells behave upon encountering bacteria," Nizet said. "In our studies with staph bacteria, the net effect of statin treatment was to improve bacterial killing and extracellular trap formation. These same changes might not be so consequential for defense against less virulent bacteria that are easily susceptible to uptake and killing within phagocytes."
The research also sheds important new light on the clinical phenomenon of reduced infection severity in patients receiving statins, the scientists said. It indicates that levels of cholesterol or related lipid molecules can be sensed by white blood cells and used as signals to control their inflammatory and antibacterial activities. Nizet and Glass recommend that future research explore whether the potential of cholesterol-lowering agents combined with antibiotics can be harnessed to optimize the treatment of certain difficult infectious disease conditions.
A human neutrophil producing DNA-based extracellular traps (stained blue), entrapping the human pathogen bacterium Staphylococcus aureus (green). This is a three-dimensional structural rendering of Simvastin, a statin.
(Photo Credit: UC San Diego School of Medicine
....................................................
(Photo Credit: UC San Diego School of Medicine
....................................................
48 Hours - CBS ON BACTERIOPHAGES
48 Hours (CBS) 09-20-2002
Environment
DAN RATHER, CBS ANCHOR: I`m Dan Rather.
A simple infection leads to a potentially life-threatening illness.
Investigating "Silent Killers", 48 HOURS right now.
(BEGIN VIDEO CLIP) ANNOUNCER: What happened to Bobbie has probably happened to you.
UNIDENTIFIED FEMALE: I got a paper cut.
ANNOUNCER: But her cut led to a drug-resistant infection that`s put her life at risk.
UNIDENTIFIED FEMALE: The bug that was in there was eating these antibiotics for breakfast.
ANNOUNCER: Alfred`s foot infection wouldn`t respond to drugs.
SUSAN SPENCER, CBS CORRESPONDENT (on camera): What sort of options were the doctors presenting you with?
UNIDENTIFIED MALE: Amputation.
ANNOUNCER: Then, he heard about an alternative treatment in the most unlikely place...
UNIDENTIFIED MALE: They had no electrical power and no water.
ANNOUNCER: ... the former Soviet Union.
SPENCER: This strikes me as fairly low-tech. Do you use these more than once?
UNIDENTIFIED FEMALE: Yes.
ANNOUNCER: Can this old technology provide new hope?
Susan Spencer investigates.
Plus: It`s a potentially fatal disease that targets college kids.
UNIDENTIFIED MALE: And I have seen young people come in with a sore throat and be dead within 24 hours.
ANNOUNCER: John was a rising star who fell fast.
PETER VAN SANT, CBS CORRESPONDENT (on camera): John, just how close were you to dying?
UNIDENTIFIED MALE: As close as you can get.
UNIDENTIFIED FEMALE: I remember falling to my knees, saying, `My God, what`s happening. What`s wrong?` ANNOUNCER: But there`s a simple vaccine that can protect your child.
Peter Van Sant with a story every parent must see. What you need to know about these growing threats.
UNIDENTIFIED MALE: And people are dying. More and more people are dying.
ANNOUNCER: "Silent Killers." (END VIDEO CLIP) RATHER: It seems incredible to think that something as common as a paper cut could somehow turn into a life-threatening condition, but it`s an indication of just how vulnerable we can be.
Good evening.
Not so long ago, it seemed modern medicine might actually eliminate the threat of infectious disease. Not so fast. Instead, our microscopic enemies, in the form of viruses and bacteria, are suddenly on the march again -- potential "Silent Killers" in the air, water and food.
One especially notable example: the West Nile virus. Unheard of in this country five years ago, is now spreading by mosquito, and will kill an estimated 100 Americans this year. No cure in sight, and officials are now worried the virus might be spread through blood transfusions. So, they are considering whether blood donors should be tested.
Tonight, some of the newest risks we`re all facing that we can`t even see. We start with Susan Spencer and one mind-boggling case, and a search for answers that leads halfway around the world.
(BEGIN VIDEOTAPE) BOBBIE MACKEON, NURSE PRACTITIONER: Sit.
SPENCER (voice-over): Two years ago, Bobbie Mackeon experienced an incredibly trivial event.
MACKEON: I got a paper cut.
SPENCER (on camera): Literally, just a paper cut.
MACKEON: Yes.
SPENCER: Deep?
MACKEON: Not that deep. And I was like, `Son of a gun.` SPENCER (voice-over): Just a paper cut.
MACKEON: You know, I washed the hands and held a little pressure on it. It stopped bleeding, and I thought, `OK.` SPENCER: But it got infected.
MACKEON: And then, this part of the finger got red and swollen.
Good boy!
SPENCER: Bobbie, a nurse practitioner, spoke with the doctors at her hospital, and they all figured an antibiotic would take care of it. It didn`t.
MACKEON: Three or four days later, it should have been looking a lot better, but it was looking worse.
SPENCER: Nor did the next two antibiotics she tried.
(on camera): This is a paper cut!
MACKEON: I know!
SPENCER: How is this possible?
MACKEON: Oh, resistant bacteria. The bug that was in there was eating these antibiotics for breakfast.
The IV line went in here.
SPENCER (voice-over): With her infection still raging, Bobbie turned to an intravenous antibiotic, which finally did help. But complications then led to potentially fatal blood clots.
MACKEON: And the blood clot was about four inches across, and it had little bubbles around it, which told us it was infected.
SPENCER: Clots so severe that her life now depends on high doses of blood thinners, and that creates new problems.
MACKEON: If I fall or hit my head or get a cut, it can be life- threatening.
SPENCER (on camera): So, you feel like you`re sort of walking on eggshells.
MACKEON: Yes.
SPENCER (voice-over): So, instead of running, like she used to, Bobbie works out ever so carefully in her garage.
MACKEON: So, I don`t want to get heart disease, because they can`t fix it. I can`t have any surgeries.
SPENCER: That a tiny infection could spiral into a life-threatening condition hardly surprises Michael Shnayerson or Mark Plotkin.
MARK PLOTKIN, CO-AUTHOR, "THE KILLERS WITHIN": I would say that the bad news is the bad bugs are getting badder faster. They`re getting stronger faster.
SPENCER: In their new book, "The Killers Within," they explore why antibiotics just don`t work like they used to.
UNIDENTIFIED MALE: Scientists are manufacturing this wonder drug in enormous quantities.
SPENCER: Shnayerson warns: MICHAEL SHNAYERSON, CO-AUTHOR, "THE KILLERS WITHIN": We no longer live in a time when antibiotics work 100 percent of the time, and, in fact, there are some bugs that are resistant to all of the antibiotics used against them. And people are dying. More and more people are dying.
SPENCER: Even the common staph infections, once easily cured, now can kill. And we`re all to blame. Like all living things, bacteria adapt to their environment. Faced with an antibiotic, a few hearty bugs survive.
Those "superbugs" then multiply, creating a new strain that the old antibiotic can`t touch.
SHNAYERSON: They are the ultimate Darwinian survivors.
SPENCER: The more antibiotics, the more the crafty critters evolve.
And for five decades, we`ve been using gobs of these drugs.
SHNAYERSON: Too many doctors still feel that antibiotics basically do no harm, and that it`s better to give them than not.
SPENCER: Plus, patients demand them, even for colds, which are viral infections against which antibiotics are useless.
And adding to overuse is agriculture. Farmers use antibiotics in feed, mostly to make the animals grow a little faster.
PLOTKIN: A recent study estimates that 70 percent of all antibiotic use in this country is used in farms.
DAVID WITT, INFECTIOUS DISEASE SPECIALIST: Indeed, I think we`re looking at the end of the antibiotic era if we don`t start changing our behavior.
SPENCER: Bobbie Mackeon`s colleague, Dr. David Witt, is an infectious disease specialist at Kaiser Permanente in California. He is also worried.
WITT: For 50 years, these were miracle drugs. They ended the major causes of death of our parents, and we thought we`d always stay a step ahead.
SPENCER: But now, the superbugs, which first only showed up in hospitals, are turning up everywhere.
WITT: And for the first time, we`re seeing resistance among very common bacteria that we`ve really not seen before.
SPENCER: Most chilling, Witt says, is the rising rate of resistance in one very common bug: pneumococcus.
WITT: And this is a bacteria that causes most cases of pneumonia, most cases of ear infections, most cases of sinusitis.
SPENCER (on camera): Everybody gets something like that.
WITT: Everybody gets them. All of your kids have had them.
GAIL MULLIN, HOLLIE MULLIN`S MOTHER: Big girl!
SPENCER (voice-over): When Gail Mullin`s three-and-a-half-week-old daughter, Hollie, got her first ear infection...
MULLIN: Oh, my goodness!
SPENCER: ... Gail, like many mothers, told the doctor just what she wanted.
MULLIN: Her ear is pink, she`s crying. So, if antibiotics can possibly solve the problem, let`s go ahead and give them to her, and he did.
Tell me all about it.
SPENCER: But more infections followed.
MULLIN: Oh, my goodness!
Hollie must have been about three months old there, and that was a pretty common face for Hollie at that age.
SPENCER (on camera): Oh, really?
MULLIN: Poor thing.
SPENCER (voice-over): And the antibiotics kept coming.
(on camera): Amoxicillin, augmentin, zithromax, receptin...
(voice-over): Seventeen different courses in one year.
MULLIN: Seven hats. Count, one, two, three...
SPENCER: By the time Hollie was 18 months old, she had developed a bacteria resistant to every oral antibiotic available.
MULLIN: I mean it was just like -- it just slapped me in the face.
SPENCER: Her only hope was a drug called Vancomycin, a potent antibiotic given intravenously.
MULLIN: And they had to surgically put it in, and it went from the crook of her arm into her chest cavity.
SPENCER: And the doctor was brutally honest. He told her: MULLIN: "This is it; this is all we have left. We don`t have any other options for her." So, you know, we knew at that time things were critical.
SPENCER: Vancomycin did work. Hollie Mullin was lucky.
(on camera): Did it make you better? And how are your ears now?
HOLLIE MULLIN: Fine.
SPENCER: There they are.
(voice-over): And her parents learned a tough lesson.
MULLIN: By giving Hollie as many antibiotics as we did, by the time she was 1 year old, we created a superbug. We created a bacteria in her system that couldn`t be beat.
SPENCER: It was Vancomycin that saved nurse Bobbie Mackeon as well, but now, she struggles with that blood clot.
(on camera): The major vein from your left shoulder to the middle of your chest...
MACKEON: Is gone.
SPENCER: Is gone.
MACKEON: Yes.
SPENCER (voice-over): Despite valiant efforts to regain her health, Bobbie has been unable to work for much of the past two years.
WITT: Bobbie`s case is a good example of the worst-case scenario.
SPENCER: And Dr. Witt expects to see many more such cases...
WITT: We probably need to look into this a bit more.
SPENCER: ... which is why he carefully checks and rechecks every antibiotic ordered at the hospital.
WITT: I don`t want to give the wrong impression. I love antibiotics.
They are life-saving. They are miracles, and I want to save them for when we need them.
SPENCER (on camera): There is some good news. A new study finds that doctors are ordering fewer antibiotics for children, but experts estimate that there still are tens of millions of unnecessary prescriptions being written each year, and the superbugs already are out there.
(voice-over): Now, even Vancomycin, that drug of last resort, is losing its punch.
(on camera): So, the idea that we potentially could lose antibiotics as a weapon...
WITT: Is chilling. It`s something that must be prevented.
SPENCER (voice-over): But could there be alternatives to antibiotics?
(on camera): So, you put the phage in there, and the bacteria is simply gone.
MZIA KUTATELADZE, ELIAVA INSTITUTE: Yes, yes, after three or four hours.
SPENCER: Wow!
SPENCER (voice-over): Next: How old technology from the former Soviet Union may hold a surprising answer.
(END VIDEOTAPE) (COMMERCIAL BREAK) (BEGIN VIDEOTAPE) SPENCER (voice-over): After breaking his foot five years ago, Toronto bass player Alfred Gertler got an infection that antibiotics couldn`t cure, and thought he might be playing the blues forever.
(on camera): What sort of options were the doctors presenting you with?
ALFRED GERTLER, MUSICIAN: Amputation.
SPENCER: Ouch.
(voice-over): But then, he read about a radically different way to treat infections. Just one catch: it was in the former Soviet Republic of Georgia, half a world away, at the Eliava Institute.
GERTLER: It was very strange, but it seemed like a lifeline, and I wanted to live. I wanted to get up and work again.
SPENCER: He went.
GERTLER: I mean, they had no heat, no electrical power and no water for much of the day.
SPENCER: What Eliava did have was treatment that worked.
(on camera): They literally took this stuff and poured it in the wound.
GERTLER: Yes. And within three days, the infection was totally gone.
SPENCER: The "stuff" they use here at the Eliava Institute is called "bacteriophage," or "phage" as some say it. Regardless of how you pronounce it, the researchers here are absolutely convinced that phages are a fine natural alternative to antibiotics. Why? Because these harmless little viruses have only one purpose in life: to eat the bacteria that cause infection.
SHNAYERSON: A miracle apparently of nature is that there seems to be a bacteriophage for every kind of bacteria.
SPENCER (voice-over): And, say the authors of "The Killers Within," these viruses may work when antibiotics fail.
PLOTKIN: Given the fix that we`re in with the rise of resistance, we need to look at other approaches, and phage is just one of several.
SPENCER: This approach is nothing new at Eliava, where they have been making phage medication for more than 60 years. Using techniques that hardly are cutting-edge, they isolate bacteria, and then search for the specific phages that kill them.
(on camera): So, you have put bacteria on this dish, and then dropped...
KUTATELADZE: Yes, the phage.
SPENCER: ... phages on it.
KUTATELADZE: Yes.
SPENCER: And...
KUTATELADZE: The clear zones are phage.
SPENCER: Which means it`s just wiped out the bacteria.
KUTATELADZE: Yes.
SPENCER (voice-over): Mzia Kutateladze is a senior scientist at the institute.
(on camera): OK, so the cloudy stuff is...
KUTATELADZE: Bacteria salmonella.
SPENCER: So, you put the phage in there, and the bacteria is simply gone.
KUTATELADZE: Yes, yes, after three or four hours.
SPENCER: Wow!
(voice-over): In local hospitals, doctors use phages to treat wounds; in clinics, to treat throat infections. For burns, there is phage bio- derm, artificial skin with time-release medication.
(on camera): So, if I go into a pharmacy in Georgia...
KUTATELADZE: Yes.
SPENCER: ... I can now buy phage treatment.
KUTATELADZE: Yes, you can.
SPENCER: And this is just accepted. Everybody knows what this is, and it`s...
KUTATELADZE: Yes, everybody knows, and it`s just a standard part of health care.
SPENCER: No big deal.
KUTATELADZE: No.
So, this is the ampules for pure phage.
SPENCER (voice-over): The price is no big deal either.
KUTATELADZE: $2.50.
SPENCER (on camera): About $2.50.
KUTATELADZE: For ten -- ten ampules.
SPENCER: For ten?
KUTATELADZE: Yes.
SPENCER: So, if I had a staph infection, I would need one box, so that would be $2.50?
KUTATELADZE: Yes, it`s very cheap in comparison to antibiotics.
SPENCER: That`s amazing.
KUTATELADZE: Yes.
SPENCER: But if phages really are all that great, why aren`t doctors in the U.S. using them, just like the doctors here? The answer to that in a word: penicillin.
UNIDENTIFIED MALE: America is continually increasing its output of penicillin, the new drug that affects almost miraculous cures.
BETTY KUTTER, MICROBIOLOGY PROFESSOR, EVERGREEN UNIVERSITY: Nobody cared very much once penicillin came along in the western world. They thought they had the problem licked for all time. We have a lot of hubris a lot of time.
SPENCER (voice-over): Betty Kutter, a microbiology professor from Evergreen University and a frequent visitor to Eliava, believes passionately that phage therapy works.
KUTTER: So, this one is sensitive.
SPENCER: She hopes to convince others that using a naturally- occurring virus to fight an infection is a fine idea.
KUTTER: These are viruses that absolutely cannot infect human cells or animal cells or plant cells.
SPENCER (on camera): No chance of getting sick from the treatment.
KUTTER: No chance of getting sick from the treatment. The only kinds of cells they can infect are bacterial cells.
Here is Alfred.
SPENCER (voice-over): It was Kutter who brought a desperate Alfred Gertler here.
(on camera): In all honesty, where do you think Alfred Gertler would be today if he had not come here?
KUTTER: He would not have a foot.
GERTLER: Oh, yes, I`m so lucky.
SPENCER (voice-over): Despite Alfred`s happy outcome...
GERTLER: It turned out great. They did what they promised to do.
SPENCER: ... his treatment would be off-limits in Canada, or in the United States, because phage therapy never has gone through the rigorous testing the U.S. demands. Eliava`s methods hardly would pass.
(on camera): This, for example, this strikes me as fairly low-tech.
KUTATELADZE: Yes, yes, it`s very old really.
SPENCER: That`s pretty old?
KUTATELADZE: Yes.
SPENCER: You use those more than once?
KUTATELADZE: Yes, we sterilize it several times.
SPENCER (voice-over): And consider where phages are found.
KUTATELADZE: We isolate the new phage clones from sewage. Yes, it`s not a very clean place...
SPENCER (on camera): It`s not appealing either.
KUTATELADZE: ... but it has a lot of phages, so.
SPENCER: Imagine you were trying to convince an American...
KUTATELADZE: Yes.
SPENCER: ... to try a medicine that was made from sewage that had viruses in it that was used in the former Soviet Union.
KUTATELADZE: Yes, but you can trust somehow, because it works. And it has been working during so much time, so.
SPENCER (voice-over): And now, some American entrepreneurs think it`s time to give this old technology new consideration.
GLENN MORRIS, INFECTIOUS DISEASE SPECIALIST: Essentially, we`re using things that nature made, but we`re kind of adding a little high-tech.
SPENCER: Infectious disease specialist, Glenn Morris, is co-founder of Intralytix in Baltimore...
MORRIS: And so, what we do is to try to fully characterize the little fellows.
SPENCER: ... one of a few small companies starting controlled studies.
MORRIS: There is no question that on the test tube and on the culture plate, these things work like gang busters. Translating that into something that`s effective in terms of human therapy, there`s a lot to suggest that they do work. But at least in this country, we still have to prove it.
SPENCER: And that will take at least three to five years, he says, even using Eliava`s experience. And who knows where Eliava will be then?
(on camera): It`s a very impressive building.
KUTATELADZE: Yes, it is.
SPENCER (voice-over): The collapse of the Soviet Union cut off funding for research, equipment and workers. Today, Eliava struggles just to hang on to its one-of-a-kind phage inventory.
KUTATELADZE: We have some experience, and maybe other people from the world, from foreign countries, can use it.
SPENCER (on camera): When you say that, a big smile comes on your face, like...
KUTATELADZE: Yes, I hope so.
SPENCER (voice-over): There has been recent outside help...
(on camera): And this is your new equipment?
KUTATELADZE: Yes, this is our new equipment.
SPENCER (voice-over): ... including a grant from the U.S. State Department.
KUTATELADZE: So, it`s very helpful, and this is the only way to save our science and just keep going.
SPENCER: No one, not even in Georgia, thinks phages will replace antibiotics completely. But are they part of the answer when antibiotics don`t work?
KUTTER: I think we are absolutely crazy if we don`t learn to use them and to use them well and efficiently and effectively.
UNIDENTIFIED FEMALE (singing): It`s very clear, our love is here to stay...
SPENCER: One Toronto musician is convinced phages saved him, for though Alfred Gertler still needs surgery to repair broken bones, he is back on his feet and playing his heart out.
(on camera): How happy are you that you took this risk and went to Georgia and did this?
GERTLER: Well, I am thrilled. Like, I am not afraid anymore. I don`t have any despair. You know, there is medicine there. So, my prospects have suddenly improved.
(END VIDEOTAPE) (BEGIN VIDEO CLIP) UNIDENTIFIED FEMALE: Drew, fruit tonight.
ANNOUNCER: Just ahead: Children and their parents who live in fear.
UNIDENTIFIED FEMALE: A sticker. Show them what it says.
Anything related to milk, he can`t have it. Even being around eggs causes him to swell up.
ANNOUNCER: Why are potentially fatal food allergies on the rise?
UNIDENTIFIED FEMALE: "NDS" in our house is "not Drew-safe." UNIDENTIFIED MALE: Yes.
ERIN MORIARTY, CBS CORRESPONDENT (on camera): He could die?
UNIDENTIFIED FEMALE: He could. Yes, he could.
(END VIDEO CLIP) (COMMERCIAL BREAK) (BEGIN VIDEOTAPE) ADRIENNE RANDALL, DREW RANDALL`S MOTHER: Drew, fruit tonight. What do you want? I`ve got blueberries, nectarines bananas.
MORIARTY (voice-over): Whenever 3-year-old Drew Randall is invited to a party near his home in Mansfield, Ohio, his mother, Adrienne, packs him food.
DREW RANDALL, SUFFERS FROM SEVERE FOOD ALLERGIES: This!
A. RANDALL: I can`t be sure that the ones that they are going to have at the party tonight are OK, so I`ll take his.
MORIARTY: Adrienne, a special education teacher, isn`t just being picky or even overprotective. A bite of the wrong food could kill Drew.
A. RANDALL: The worst-case scenario is that he has an anaphylactic reaction that causes some kind of, like, terminal damage.
MORIARTY (on camera): He could die?
A. RANDALL: He could. Yes, he could.
MORIARTY (voice-over): Drew has severe food allergies.
A. RANDALL: He`s sensitive enough to egg that even being around eggs when they`re cooking causes him to swell up. He`s allergic to milk, and then he`s also allergic to peanuts.
JACQUI CORBA, SUFFERS FROM SEVERE FOOD ALLERGIES: I have trouble breathing, my throat feels tight.
MORIARTY: Twelve-year-old Jacqui Corba of Greenwich, Connecticut, is also allergic to peanuts. She can`t eat them or even inhale the dust from them.
J. CORBA: It feels like you`re scared that you`re going to die.
MORIARTY: And it`s not just peanuts.
J. CORBA: Sesame seeds, pumpkin seeds, sunflower seeds, poppy seeds.
MORIARTY (on camera): Eating something that was made in a factory that processes peanuts?
J. CORBA: That could -- that could kill me.
MORIARTY: Kill you?
J. CORBA: Yes.
MORIARTY: Anyone who has a child today knows someone like Jacqui and Drew. There are an estimated seven million Americans with food allergies, with an average of 200 who die every year. And while no one knows exactly why, the number of those with food allergies is on the rise.
DR. HUGH SAMPSON, ALLERGIST: There does appear to be almost an epidemic, I would say, in the last five to 10 years.
MORIARTY (voice-over): Dr. Hugh Sampson is an allergist at Mt. Sinai Hospital in New York.
(on camera): Why are we seeing so many more kids with food allergies?
SAMPSON: That`s a great question.
MORIARTY (voice-over): First and foremost, there seems to be a link between nursing mothers and eating peanuts. It may not be a coincidence, says Dr. Sampson, that 90 percent of the children who develop a serious peanut allergy, including Drew and Jacqui, were breastfed as infants.
SAMPSON: With the increase in breastfeeding, some of these children are getting exposed to very allergenic proteins. The general consensus is, we`d rather the mothers not eat peanuts while they`re breastfeeding if they`re from allergic families.
MORIARTY: This is one of Dr. Sampson`s young patients during a test for an allergy to egg.
SAMPSON: And then, you can see when we look on the rest of his body, he`s got, you know, a very itchy, red rash.
You`re really doing Russian roulette. You know, you spin the barrel each time you have a reaction, and I think that`s what generates such fear in the parents.
MORIARTY: Jacqui Corba has already had 15 allergic episodes.
J. CORBA: When we went outside...
MORIARTY: Because each one seems more severe than the last, Jacqui`s life has become ruled by food -- what she can eat and what she can`t.
DIANE CORBA, JACQUI CORBA`S MOTHER: Like, this is the nightmare right here, this section.
MORIARTY: Grocery shopping for Jacqui`s mom, Diane, has become an unpleasant, even scary ordeal.
D. CORBA: Allergy information, there it is. I`m going to look all through this.
MORIARTY: While many food manufacturers have added allergy information to their labels, and Congress is considering a law that would make it mandatory, in some cases, a silent killer is invisible.
D. CORBA: Now it says "pecans." MORIARTY (on camera): And what does it say on the allergy information?
D. CORBA: It doesn`t say anything about nuts, which is very weird.
That`s why you have to read it.
MORIARTY: Because, if you make a mistake, yes.
D. CORBA: So much for that label.
A. RANDALL: Pop tart big.
D. RANDALL: Yes.
MORIARTY (voice-over): Life is even more complicated for Adrienne Randall, whose 3-year-old son, Drew, has an even greater number of food allergies.
A. RANDALL: This cabinet is all Drew-safe. Everything in here is stuff that`s either for Drew or that Drew can eat.
MORIARTY: Because her older son, 4-year-old Jake, doesn`t have any allergies, Adrienne has had to devise a complex storage system to keep their food separated.
(on camera): What does that "NDS" mean?
A. RANDALL: This means, "not Drew-safe." This is the stuff that Jacob can pull out, like, for a snack if Drew is not around.
I have "not Drew-safe" on the top, and then, I always write it on the ingredients panel.
MORIARTY (voice-over): But keeping things safe is getting more and more difficult the older Drew gets and the more places he eats, like birthday parties.
A. RANDALL: Your sticker to remind people that they should not feed you, right? Why not? Why do they not feed you?
D. RANDALL: Because I could get sick.
MORIARTY: But even with the plainly visible sticker, Adrienne still hovers nearby.
A. RANDALL: I`m waiting to eat. Then, I won`t be so nervous.
MORIARTY: While Drew is too young to care, Jacqui knows what it`s like to be singled out for her allergy. A talented tennis player who hopes one day to play professionally, she`s best known at her middle school as: J. CORBA: "Peanut Girl." That`s me. That`s the popular one.
"Peanut Girl." MORIARTY (on camera): And how do you feel about it?
J. CORBA: I can`t stand it.
MORIARTY (voice-over): Because Jacqui`s food allergy is considered a disability, her school is required by law to keep her safe. So, at lunch, Jacqui eats in what`s called a "peanut-free zone" that includes not only her table, but the ones that surround hers.
(on camera): So you like her that much that you`ll give up that Snickers bar?
(voice-over): And even with all of the precautions, Jacqui never leaves home without her epi-pens...
(on camera): This is, like, a shot.
J. CORBA: Yes.
MORIARTY: Where does it go?
J. CORBA: It goes right in my leg.
MORIARTY (voice-over): ... disposable syringes that carry medicine, epinephrine. That could save her life in the event of a severe allergic reaction, like the one she had a year-a-half ago in a New York deli.
J. CORBA: And my mom and I asked, "So, does this have any seeds on the bun?" And they said, "No." I was about to take another bite, and I looked on the bottom, there was about four seeds.
MORIARTY: Thirty minutes later, Jacqui was in serious trouble.
D. CORBA: I saw her, and she was like gray and like the cupboard.
And she started sliding down the wall, and I just grabbed the epi-pen and just jammed it in her leg.
MORIARTY: Diane rushed Jacqui to the hospital.
D. CORBA: I think that it was the worst time of her life, but clearly, the worst time of my life. I mean, just to be in the middle of that and know that this is going to happen again.
MORIARTY (on camera): After that experience, were you hesitant to eat food at all?
J. CORBA: I was so hesitant. I -- it changed me. It changed me. I was very, very nervous to eat.
MORIARTY (voice-over): And Jacqui is still nervous.
J. CORBA: I get so nervous and full of anxiety that I create the symptoms. I still get a little shaky in New York, like eating. I don`t want to get near that street. It just scares me. I don`t want to look at that hospital.
MORIARTY: Because only 20 percent of children with peanut allergies outgrow them, Jacqui is going to have to get used to living with anxiety, which is why playing tennis has come to mean so much to Jacqui. On the court, her only risk is losing a match.
(on camera): And when you`re playing tennis, you`re not the "Peanut Girl?" J. CORBA: And I love that.
MORIARTY: You`re not worrying about your allergies?
J. CORBA: Yes, I just play my game, and it`s peaceful. It`s a great feeling to know that I don`t have to worry about that situation.
(END VIDEOTAPE) (BEGIN VIDEO CLIP) ANNOUNCER: Next: One family`s heartbreaking journey.
VAN SANT (on camera): John, just how close were you to dying?
UNIDENTIFIED MALE: As close as you can get.
UNIDENTIFIED FEMALE: I remember falling to my knees saying, `My God, what`s happening? What`s wrong?` ANNOUNCER: But it might easily have been prevented. We`ll show you how.
(END VIDEO CLIP) (COMMERCIAL BREAK) RATHER: Millions of college students have been arriving on campuses all across the country, armed with the latest tools for the information age -- laptops, cell phones, pagers and Palm Pilots -- all at the ready. But there is something else going around on campus that a lot of students and their parents may not be prepared for, although it is something a lot of medical experts say young people can and should be protected against.
Peter Van Sant now has a story of one family who got a lesson they never anticipated.
(BEGIN VIDEOTAPE) JOHN KACH, COLLEGE STUDENT: Everything was, you know, going my way.
I was happy.
VAN SANT (voice-over): In March of 2000...
J. KACH: I started concentrating on basketball, started to lift, getting my grades up, still parties, still doing my thing.
VAN SANT: ... 19-year-old John Kach was having the time of his life.
A college freshman at Salve Regina University in Newport, Rhode Island, John was on his way to becoming a star basketball player.
(on camera): What`s this picture?
J. KACH: This is when we beat Bridgewater State, I had basically the game-winning basket.
VAN SANT (voice-over): But just months after that winning basket, this 6 foot 4, 210-pound athlete lost almost everything.
John`s nightmare began when he was recovering from what he thought was the flu...
J. KACH: I was in my dorm room on a Friday night. I wasn`t feeling all that great, so I stayed in. All of a sudden, my stomach doesn`t feel right. And you know, and then I started getting real hot, fever.
VAN SANT: ... until John`s fever soared to 105, and he was rushed to the hospital.
PAIGE KACH, JOHN KACH`S MOTHER: To be that sick, to be brought to the hospital, knowing my son, John, it just gave me that funny feeling.
VAN SANT: John`s mother, Paige, was more than 150 miles away at her home in Carmel, New York, when she got a call from an emergency room doctor.
P. KACH: And he said, "Mrs. Kach, we are transporting John from Newport Hospital to Providence. He`s a very, very sick young man, and you`ve got to get here as soon as you can." I remember falling to my knees saying, `My God, what`s happening?
What`s wrong?" VAN SANT: John had contracted a rare, but often fatal form of bacterial meningitis that attacked and shut down his major organs.
DR. MITCHELL LEVY, INTENSIVE CARE SPECIALIST: There`s very little warning, and if you don`t see someone very early, it can be difficult to prevent death.
VAN SANT: Intensive care specialist, Dr. Mitchell Levy of Rhode Island Hospital, was battling the meningitis with massive amounts of antibiotics.
LEVY: His lungs were filling up with fluid, and his blood pressure was gravely low.
VAN SANT: Unable to breathe on his own, John was placed into a drug- induced coma. Within the first two days, John was given his last rites not once, but twice.
P. KACH: I remember going into John`s room, and he was under. And I remember kissing him and saying, `If you can`t do this, if you can`t make it through this, you go ahead and go. Mommy will understand. Don`t stay for mommy, because I`ll understand. But if you want to do this and you want to fight, we will fight this as a family.` VAN SANT (on camera): John was fighting a disease he most likely caught at college. Bacterial meningitis is spread through saliva, and studies show that college freshmen living in dorms are in the highest risk group.
LEVY: Why eight people can be exposed to it and only one person gets it is still a mystery to medicine. And I have seen young people come in with a sore throat and be dead within 24 hours.
VAN SANT (voice-over): And each year, more than 100 college freshmen, like John, come down with the disease.
LEVY: I thought he was going to die. I thought he was going to die, and not just when he first came in, but honestly, for quite a while after he was in the ICU.
VAN SANT: Weeks passed, and the Kach family camped out in the hospital waiting room.
(on camera): And how close are you to your brother?
MIKE KACH JR., JOHN KACH`S BROTHER: Real close.
VAN SANT: So, he`s a good friend as well as a brother?
M. KACH JR.: Best friend.
VAN SANT (voice-over): John`s 19-year-old brother, Mike Jr., remembers those painful days.
M. KACH JR.: It was like a dream. It didn`t seem like it was real.
I just waited.
VAN SANT: John`s father, Mike Sr., watched as his son wasted away.
(on camera): Give me a sense, Michael, of the shock of seeing your son, the athlete, in bed with that mask on?
MIKE KACH SR., JOHN KACH`S FATHER: Not shock as much as fear -- just pure, pure fear.
VAN SANT (voice-over): To keep their hope alive, John`s family and friends kept a journal.
P. KACH: All of your teammates have been here, and Mike has been here every day.
M. KACH JR.: "You`re my best friend and my idol. I have looked up to you since I was a little kid. I love you. Mike." VAN SANT: After six weeks of treatment, Dr. Levy decided to bring John out of the coma.
J. KACH: When I woke up, I remember Dr. Levy leaning over me, slapping his hands.
LEVY: You clapped, and you said, "John, look at me." P. KACH: It was probably one of the happiest days of my life.
M. KACH JR.: I kissed him. I said, I loved him, because that was what I was waiting to say to him the whole time. He asked me how school was going, how basketball was going. I mean, he always cared so much for me that he would always ask me how I was doing, when he was the one laying in the bed.
VAN SANT: But John`s physical ordeal was just beginning. Doctors were able to save his life, but the price was very high.
MIKE KACH SR.: I have never really begged for anything in my life, but I did beg the doctor, `Please, be as conservative and frugal as you possibly can.` VAN SANT (on camera): What are we looking at here?
J. KACH: This is my right leg. This is the one that I lost below my knee.
VAN SANT: And what are we looking at here?
J. KACH: That`s my right hand.
VAN SANT: What goes through your mind when you look at this?
J. KACH: It`s tough. You know, it`s tough to think that that`s me.
VAN SANT: That`s your right hand in this picture, and let me see your right hand now.
J. KACH: That`s my right hand today.
VAN SANT (voice-over): The meningitis prevented blood from circulating to John`s limbs, causing tissue to die. Amputation was inevitable.
P. KACH: Any parent sitting anywhere can`t even imagine how horrible it is to have somebody say, "We`re going to cut off his hands, we`re going to cut off his legs." You`re a beautiful child. You`re a gorgeous 6 foot 4, strapping, 210, handsome young man, who walks and runs and plays and jumps around and holds hands with his girlfriend. And all of a sudden, you`re going to take all of that away?
VAN SANT: What the disease couldn`t take away was John`s will.
J. KACH: It was a lot of pain. I think I could go through anything right now.
VAN SANT: He triumphed over five grueling months in rehab.
P. KACH: He said to me once, "Why me, Ma? I tried to do it all by the book. Why me?" I had no answers. I said, `Honey, I don`t know.` And he never asked me that again.
UNIDENTIFIED MALE: You can do the honors.
UNIDENTIFIED MALE: What is that?
VAN SANT: Today, with the help of his family, and these custom-made pads for his hands...
J. KACH: And my dad just made them up to fit me better. And with these, you know, I can squeeze the ball.
VAN SANT: ... John has learned to do just about everything.
P. KACH: I think he was born with something so special, and I think we were lucky enough to nurture it.
VAN SANT: As terrible as what happened to John Kach, it`s almost as agonizing to know...
J. KACH: I knew about the vaccine, didn`t get it, wish I did.
VAN SANT: ... it might easily have been prevented.
P. KACH: There is a vaccine that can prevent this kind of heartache.
VAN SANT: That`s next.
(END VIDEOTAPE) (COMMERCIAL BREAK) (BEGIN VIDEOTAPE) UNIDENTIFIED MALE: One, two, lock it. Give me one more. Come on, push, push. Come on, come on.
VAN SANT (voice-over): John Kach is working hard to rebuild his life...
UNIDENTIFIED MALE: Good.
VAN SANT: ... and his body...
UNIDENTIFIED MALE: Come on, push. Good.
VAN SANT: ... which were both nearly destroyed by bacterial meningitis.
(on camera): John, just how close were you to dying?
J. KACH: As close as you can get.
VAN SANT (voice-over): John`s close encounter with death has set him on a new mission: To let people know that most forms of the disease can be prevented with a single shot.
J. KACH: I`m here today to talk with my mom to basically get the word out about the vaccine.
VAN SANT: John and his mother, Paige, are part of a group called, Moms on Meningitis. Their message: What happened to John doesn`t have to happen to you.
J. KACH: This changed my life big-time. And you know, I don`t want to see anyone else go through what I went through and my family went through. I wouldn`t wish this on my worst enemy.
DR. JAMES TURNER, UNIVERSITY OF VIRGINIA: If you get the shot, you have reduced your risk by about 80 percent.
VAN SANT: Dr. James Turner is the executive director of student health at the University of Virginia, where all incoming freshmen are required to be vaccinated for bacterial meningitis.
TURNER: We have learned of a lot of young people`s lives who could have been saved if we had only been vaccinating years ago.
VAN SANT: The vaccine was first developed in the 1960s, after a series of meningitis outbreaks in crowded military barracks.
TURNER: About 1971, every single military recruit started receiving this vaccine, and the outbreaks of the disease virtually stopped.
VAN SANT (on camera): Today, it`s crowded college dormitories that are the breeding ground for the disease. Each year, about 100 students get sick, and a dozen die of bacterial meningitis.
Five states now mandate that all incoming freshmen be vaccinated. The cost: between $70 and $80 per student.
TURNER: It`s a god-awful disease, and I have sat in the intensive care units with the families as they have watched their children cling to life, and it`s terrible. And to think for $70 or $80, we can prevent that, it`s a no-brainer.
VAN SANT (voice-over): With virtually no side effects, Dr. Turner wants to make the shot mandatory in all 50 states.
TURNER: We have made tremendous headway in getting students vaccinated and getting information out there. Clearly, we`ve got a ways to go.
UNIDENTIFIED MALE: Nothing makes me more excited than being able to announce No. 25, John Kach.
VAN SANT: John Kach doesn`t dwell on the past. Just nine months after getting sick, John made an emotional return to visit his former teammates.
J. KACH: I just try to make my life better, people`s lives around me better, and just kind of show them, you know, there`s a lot to live for.
VAN SANT (on camera): All right, man. Show me what you`ve got.
(voice-over): Today, John is not giving up his favorite sport. He`s in training with a new goal: to make the U.S. Para-Olympic basketball team.
(on camera): Well, I`ll tell you, with all that you have been through, it`s a privilege to shoot hoops with you in this gym, man.
J. KACH: Thank you.
VAN SANT: It`s really a privilege.
(END VIDEOTAPE) (BEGIN VIDEO CLIP) ANNOUNCER: A paper cut nearly killed Bobbie Mackeon. What are her chances for a full recovery? Stay with us.
(END VIDEO CLIP) (COMMERCIAL BREAK) (BEGIN VIDEOTAPE) UNIDENTIFIED FEMALE: So, go ahead, bring your arms up above your head.
UNIDENTIFIED MALE: Breathe in. Hold your breath.
SPENCER (voice-over): Nurse Bobbie Mackeon is still struggling to overcome serious medical problems from an infected paper cut.
MACKEON: Ten years ago, we would have treated it with one drug, it would have been gone. But unfortunately, the bacteria have gotten smart.
SPENCER: In her case, oral antibiotics failed, and more drastic treatment left her with life-threatening complications.
MACKEON: I still have the pain in here that doesn`t seem to go away.
Some days are worse than others SPENCER: But today, there is good news. Her condition seems to have stabilized.
MACKEON: I can lower the amount of blood thinner I`m on.
SPENCER: And she can start working part-time.
MACKEON: I missed my patients.
SPENCER: She says, she won`t hesitate to drive home with her patients the lesson that she learned firsthand: Overuse antibiotics, and they soon may have no use at all.
MACKEON: If I can get them to understand why I don`t want to give an antibiotic for a virus, maybe my grandchildren will have antibiotics that work.
(END VIDEOTAPE) RATHER: Tonight is the last 48 HOURS I`ll be doing, at least for a while. It`s been a long, good run; more than 15 years, as one who helped create the program, and then be a reporter and anchor for it.
The original idea was to be on once a week or more in primetime, with focused, emotionally moving hours of television journalism that affects people`s lives. Not just short bursts, but full hours on one subject. And to do full hours in times of crisis -- everything from hurricanes to war.
48 HOURS has done that, and is today the third longest-running program in primetime. Some of the most accomplished, professional journalists in the world have made it so, and they`ll continue to do that.
In the season ahead, my friend and colleague, the veteran and distinguished correspondent, Lesley Stahl, will be anchoring the new 48 HOURS: 48 HOURS INVESTIGATES. Lesley and the 48 HOURS` team will take this broadcast proudly into the future.
And now, please, take a look at a preview of next Friday`s season premiere of "48 HOURS INVESTIGATES.
(BEGIN VIDEO CLIP) ANNOUNCER: A respected doctor is accused of using a patient for sex.
UNIDENTIFIED MALE: I am facing 18 years of prison for something I didn`t do.
ANNOUNCER: But this is no ordinary case.
UNIDENTIFIED FEMALE: Who is going to believe me?
ANNOUNCER: His accuser has been diagnosed with multiple personalities.
UNIDENTIFIED FEMALE: I don`t have a warning, and I -- and they just...
PETER VAN SANT, CBS CORRESPONDENT (on camera): They just appear?
UNIDENTIFIED FEMALE: Yes.
UNIDENTIFIED FEMALE: Who am I speaking to now?
UNIDENTIFIED FEMALE: (EXPLETIVE DELETED) man, you know. All right, hey, man, (EXPLETIVE DELETED) am only.
UNIDENTIFIED MALE: My life is at stake. My family`s life is at stake.
UNIDENTIFIED FEMALE: How do you do?
ANNOUNCER: You won`t believe this trial.
UNIDENTIFIED MALE: Am I talking to Vanessa?
ANNOUNCER: And, 48 HOURS did our own DNA testing with explosive results the jury never saw.
UNIDENTIFIED MALE: I never, ever had any kind of sexual contact with this lady.
UNIDENTIFIED FEMALE: Dr. Malave (ph) is lying.
ANNOUNCER: The season premiere of 48 HOURS INVESTIGATES, "A Crime of the Mind," next Friday.
(END VIDEO CLIP) RATHER: I`m Dan Rather.
As always, thank you for watching. And be sure to tune in next week for the season premiere of 48 HOURS INVESTIGATES.
Good night.
END
Content and programming Copyright MCMXCVIII CBS Worldwide Inc. ALL RIGHTS RESERVED. Transcription Copyright MCMXCVIII Federal Document Clearting House, Inc., which takes sole responsibility for the accuracy of the transcription. ALL RIGHTS RESERVED. This is not a legal transcript for purposes of litigation.
Content and programming Copyright 2002 CBS Worldwide Inc. ALL RIGHTS RESERVED. Transcription Copyright 2002 Federal Document Clearing House, Inc., which takes sole responsibility for the accuracy of the transcription.
A simple infection leads to a potentially life-threatening illness.
Investigating "Silent Killers", 48 HOURS right now.
(BEGIN VIDEO CLIP) ANNOUNCER: What happened to Bobbie has probably happened to you.
UNIDENTIFIED FEMALE: I got a paper cut.
ANNOUNCER: But her cut led to a drug-resistant infection that`s put her life at risk.
UNIDENTIFIED FEMALE: The bug that was in there was eating these antibiotics for breakfast.
ANNOUNCER: Alfred`s foot infection wouldn`t respond to drugs.
SUSAN SPENCER, CBS CORRESPONDENT (on camera): What sort of options were the doctors presenting you with?
UNIDENTIFIED MALE: Amputation.
ANNOUNCER: Then, he heard about an alternative treatment in the most unlikely place...
UNIDENTIFIED MALE: They had no electrical power and no water.
ANNOUNCER: ... the former Soviet Union.
SPENCER: This strikes me as fairly low-tech. Do you use these more than once?
UNIDENTIFIED FEMALE: Yes.
ANNOUNCER: Can this old technology provide new hope?
Susan Spencer investigates.
Plus: It`s a potentially fatal disease that targets college kids.
UNIDENTIFIED MALE: And I have seen young people come in with a sore throat and be dead within 24 hours.
ANNOUNCER: John was a rising star who fell fast.
PETER VAN SANT, CBS CORRESPONDENT (on camera): John, just how close were you to dying?
UNIDENTIFIED MALE: As close as you can get.
UNIDENTIFIED FEMALE: I remember falling to my knees, saying, `My God, what`s happening. What`s wrong?` ANNOUNCER: But there`s a simple vaccine that can protect your child.
Peter Van Sant with a story every parent must see. What you need to know about these growing threats.
UNIDENTIFIED MALE: And people are dying. More and more people are dying.
ANNOUNCER: "Silent Killers." (END VIDEO CLIP) RATHER: It seems incredible to think that something as common as a paper cut could somehow turn into a life-threatening condition, but it`s an indication of just how vulnerable we can be.
Good evening.
Not so long ago, it seemed modern medicine might actually eliminate the threat of infectious disease. Not so fast. Instead, our microscopic enemies, in the form of viruses and bacteria, are suddenly on the march again -- potential "Silent Killers" in the air, water and food.
One especially notable example: the West Nile virus. Unheard of in this country five years ago, is now spreading by mosquito, and will kill an estimated 100 Americans this year. No cure in sight, and officials are now worried the virus might be spread through blood transfusions. So, they are considering whether blood donors should be tested.
Tonight, some of the newest risks we`re all facing that we can`t even see. We start with Susan Spencer and one mind-boggling case, and a search for answers that leads halfway around the world.
(BEGIN VIDEOTAPE) BOBBIE MACKEON, NURSE PRACTITIONER: Sit.
SPENCER (voice-over): Two years ago, Bobbie Mackeon experienced an incredibly trivial event.
MACKEON: I got a paper cut.
SPENCER (on camera): Literally, just a paper cut.
MACKEON: Yes.
SPENCER: Deep?
MACKEON: Not that deep. And I was like, `Son of a gun.` SPENCER (voice-over): Just a paper cut.
MACKEON: You know, I washed the hands and held a little pressure on it. It stopped bleeding, and I thought, `OK.` SPENCER: But it got infected.
MACKEON: And then, this part of the finger got red and swollen.
Good boy!
SPENCER: Bobbie, a nurse practitioner, spoke with the doctors at her hospital, and they all figured an antibiotic would take care of it. It didn`t.
MACKEON: Three or four days later, it should have been looking a lot better, but it was looking worse.
SPENCER: Nor did the next two antibiotics she tried.
(on camera): This is a paper cut!
MACKEON: I know!
SPENCER: How is this possible?
MACKEON: Oh, resistant bacteria. The bug that was in there was eating these antibiotics for breakfast.
The IV line went in here.
SPENCER (voice-over): With her infection still raging, Bobbie turned to an intravenous antibiotic, which finally did help. But complications then led to potentially fatal blood clots.
MACKEON: And the blood clot was about four inches across, and it had little bubbles around it, which told us it was infected.
SPENCER: Clots so severe that her life now depends on high doses of blood thinners, and that creates new problems.
MACKEON: If I fall or hit my head or get a cut, it can be life- threatening.
SPENCER (on camera): So, you feel like you`re sort of walking on eggshells.
MACKEON: Yes.
SPENCER (voice-over): So, instead of running, like she used to, Bobbie works out ever so carefully in her garage.
MACKEON: So, I don`t want to get heart disease, because they can`t fix it. I can`t have any surgeries.
SPENCER: That a tiny infection could spiral into a life-threatening condition hardly surprises Michael Shnayerson or Mark Plotkin.
MARK PLOTKIN, CO-AUTHOR, "THE KILLERS WITHIN": I would say that the bad news is the bad bugs are getting badder faster. They`re getting stronger faster.
SPENCER: In their new book, "The Killers Within," they explore why antibiotics just don`t work like they used to.
UNIDENTIFIED MALE: Scientists are manufacturing this wonder drug in enormous quantities.
SPENCER: Shnayerson warns: MICHAEL SHNAYERSON, CO-AUTHOR, "THE KILLERS WITHIN": We no longer live in a time when antibiotics work 100 percent of the time, and, in fact, there are some bugs that are resistant to all of the antibiotics used against them. And people are dying. More and more people are dying.
SPENCER: Even the common staph infections, once easily cured, now can kill. And we`re all to blame. Like all living things, bacteria adapt to their environment. Faced with an antibiotic, a few hearty bugs survive.
Those "superbugs" then multiply, creating a new strain that the old antibiotic can`t touch.
SHNAYERSON: They are the ultimate Darwinian survivors.
SPENCER: The more antibiotics, the more the crafty critters evolve.
And for five decades, we`ve been using gobs of these drugs.
SHNAYERSON: Too many doctors still feel that antibiotics basically do no harm, and that it`s better to give them than not.
SPENCER: Plus, patients demand them, even for colds, which are viral infections against which antibiotics are useless.
And adding to overuse is agriculture. Farmers use antibiotics in feed, mostly to make the animals grow a little faster.
PLOTKIN: A recent study estimates that 70 percent of all antibiotic use in this country is used in farms.
DAVID WITT, INFECTIOUS DISEASE SPECIALIST: Indeed, I think we`re looking at the end of the antibiotic era if we don`t start changing our behavior.
SPENCER: Bobbie Mackeon`s colleague, Dr. David Witt, is an infectious disease specialist at Kaiser Permanente in California. He is also worried.
WITT: For 50 years, these were miracle drugs. They ended the major causes of death of our parents, and we thought we`d always stay a step ahead.
SPENCER: But now, the superbugs, which first only showed up in hospitals, are turning up everywhere.
WITT: And for the first time, we`re seeing resistance among very common bacteria that we`ve really not seen before.
SPENCER: Most chilling, Witt says, is the rising rate of resistance in one very common bug: pneumococcus.
WITT: And this is a bacteria that causes most cases of pneumonia, most cases of ear infections, most cases of sinusitis.
SPENCER (on camera): Everybody gets something like that.
WITT: Everybody gets them. All of your kids have had them.
GAIL MULLIN, HOLLIE MULLIN`S MOTHER: Big girl!
SPENCER (voice-over): When Gail Mullin`s three-and-a-half-week-old daughter, Hollie, got her first ear infection...
MULLIN: Oh, my goodness!
SPENCER: ... Gail, like many mothers, told the doctor just what she wanted.
MULLIN: Her ear is pink, she`s crying. So, if antibiotics can possibly solve the problem, let`s go ahead and give them to her, and he did.
Tell me all about it.
SPENCER: But more infections followed.
MULLIN: Oh, my goodness!
Hollie must have been about three months old there, and that was a pretty common face for Hollie at that age.
SPENCER (on camera): Oh, really?
MULLIN: Poor thing.
SPENCER (voice-over): And the antibiotics kept coming.
(on camera): Amoxicillin, augmentin, zithromax, receptin...
(voice-over): Seventeen different courses in one year.
MULLIN: Seven hats. Count, one, two, three...
SPENCER: By the time Hollie was 18 months old, she had developed a bacteria resistant to every oral antibiotic available.
MULLIN: I mean it was just like -- it just slapped me in the face.
SPENCER: Her only hope was a drug called Vancomycin, a potent antibiotic given intravenously.
MULLIN: And they had to surgically put it in, and it went from the crook of her arm into her chest cavity.
SPENCER: And the doctor was brutally honest. He told her: MULLIN: "This is it; this is all we have left. We don`t have any other options for her." So, you know, we knew at that time things were critical.
SPENCER: Vancomycin did work. Hollie Mullin was lucky.
(on camera): Did it make you better? And how are your ears now?
HOLLIE MULLIN: Fine.
SPENCER: There they are.
(voice-over): And her parents learned a tough lesson.
MULLIN: By giving Hollie as many antibiotics as we did, by the time she was 1 year old, we created a superbug. We created a bacteria in her system that couldn`t be beat.
SPENCER: It was Vancomycin that saved nurse Bobbie Mackeon as well, but now, she struggles with that blood clot.
(on camera): The major vein from your left shoulder to the middle of your chest...
MACKEON: Is gone.
SPENCER: Is gone.
MACKEON: Yes.
SPENCER (voice-over): Despite valiant efforts to regain her health, Bobbie has been unable to work for much of the past two years.
WITT: Bobbie`s case is a good example of the worst-case scenario.
SPENCER: And Dr. Witt expects to see many more such cases...
WITT: We probably need to look into this a bit more.
SPENCER: ... which is why he carefully checks and rechecks every antibiotic ordered at the hospital.
WITT: I don`t want to give the wrong impression. I love antibiotics.
They are life-saving. They are miracles, and I want to save them for when we need them.
SPENCER (on camera): There is some good news. A new study finds that doctors are ordering fewer antibiotics for children, but experts estimate that there still are tens of millions of unnecessary prescriptions being written each year, and the superbugs already are out there.
(voice-over): Now, even Vancomycin, that drug of last resort, is losing its punch.
(on camera): So, the idea that we potentially could lose antibiotics as a weapon...
WITT: Is chilling. It`s something that must be prevented.
SPENCER (voice-over): But could there be alternatives to antibiotics?
(on camera): So, you put the phage in there, and the bacteria is simply gone.
MZIA KUTATELADZE, ELIAVA INSTITUTE: Yes, yes, after three or four hours.
SPENCER: Wow!
SPENCER (voice-over): Next: How old technology from the former Soviet Union may hold a surprising answer.
(END VIDEOTAPE) (COMMERCIAL BREAK) (BEGIN VIDEOTAPE) SPENCER (voice-over): After breaking his foot five years ago, Toronto bass player Alfred Gertler got an infection that antibiotics couldn`t cure, and thought he might be playing the blues forever.
(on camera): What sort of options were the doctors presenting you with?
ALFRED GERTLER, MUSICIAN: Amputation.
SPENCER: Ouch.
(voice-over): But then, he read about a radically different way to treat infections. Just one catch: it was in the former Soviet Republic of Georgia, half a world away, at the Eliava Institute.
GERTLER: It was very strange, but it seemed like a lifeline, and I wanted to live. I wanted to get up and work again.
SPENCER: He went.
GERTLER: I mean, they had no heat, no electrical power and no water for much of the day.
SPENCER: What Eliava did have was treatment that worked.
(on camera): They literally took this stuff and poured it in the wound.
GERTLER: Yes. And within three days, the infection was totally gone.
SPENCER: The "stuff" they use here at the Eliava Institute is called "bacteriophage," or "phage" as some say it. Regardless of how you pronounce it, the researchers here are absolutely convinced that phages are a fine natural alternative to antibiotics. Why? Because these harmless little viruses have only one purpose in life: to eat the bacteria that cause infection.
SHNAYERSON: A miracle apparently of nature is that there seems to be a bacteriophage for every kind of bacteria.
SPENCER (voice-over): And, say the authors of "The Killers Within," these viruses may work when antibiotics fail.
PLOTKIN: Given the fix that we`re in with the rise of resistance, we need to look at other approaches, and phage is just one of several.
SPENCER: This approach is nothing new at Eliava, where they have been making phage medication for more than 60 years. Using techniques that hardly are cutting-edge, they isolate bacteria, and then search for the specific phages that kill them.
(on camera): So, you have put bacteria on this dish, and then dropped...
KUTATELADZE: Yes, the phage.
SPENCER: ... phages on it.
KUTATELADZE: Yes.
SPENCER: And...
KUTATELADZE: The clear zones are phage.
SPENCER: Which means it`s just wiped out the bacteria.
KUTATELADZE: Yes.
SPENCER (voice-over): Mzia Kutateladze is a senior scientist at the institute.
(on camera): OK, so the cloudy stuff is...
KUTATELADZE: Bacteria salmonella.
SPENCER: So, you put the phage in there, and the bacteria is simply gone.
KUTATELADZE: Yes, yes, after three or four hours.
SPENCER: Wow!
(voice-over): In local hospitals, doctors use phages to treat wounds; in clinics, to treat throat infections. For burns, there is phage bio- derm, artificial skin with time-release medication.
(on camera): So, if I go into a pharmacy in Georgia...
KUTATELADZE: Yes.
SPENCER: ... I can now buy phage treatment.
KUTATELADZE: Yes, you can.
SPENCER: And this is just accepted. Everybody knows what this is, and it`s...
KUTATELADZE: Yes, everybody knows, and it`s just a standard part of health care.
SPENCER: No big deal.
KUTATELADZE: No.
So, this is the ampules for pure phage.
SPENCER (voice-over): The price is no big deal either.
KUTATELADZE: $2.50.
SPENCER (on camera): About $2.50.
KUTATELADZE: For ten -- ten ampules.
SPENCER: For ten?
KUTATELADZE: Yes.
SPENCER: So, if I had a staph infection, I would need one box, so that would be $2.50?
KUTATELADZE: Yes, it`s very cheap in comparison to antibiotics.
SPENCER: That`s amazing.
KUTATELADZE: Yes.
SPENCER: But if phages really are all that great, why aren`t doctors in the U.S. using them, just like the doctors here? The answer to that in a word: penicillin.
UNIDENTIFIED MALE: America is continually increasing its output of penicillin, the new drug that affects almost miraculous cures.
BETTY KUTTER, MICROBIOLOGY PROFESSOR, EVERGREEN UNIVERSITY: Nobody cared very much once penicillin came along in the western world. They thought they had the problem licked for all time. We have a lot of hubris a lot of time.
SPENCER (voice-over): Betty Kutter, a microbiology professor from Evergreen University and a frequent visitor to Eliava, believes passionately that phage therapy works.
KUTTER: So, this one is sensitive.
SPENCER: She hopes to convince others that using a naturally- occurring virus to fight an infection is a fine idea.
KUTTER: These are viruses that absolutely cannot infect human cells or animal cells or plant cells.
SPENCER (on camera): No chance of getting sick from the treatment.
KUTTER: No chance of getting sick from the treatment. The only kinds of cells they can infect are bacterial cells.
Here is Alfred.
SPENCER (voice-over): It was Kutter who brought a desperate Alfred Gertler here.
(on camera): In all honesty, where do you think Alfred Gertler would be today if he had not come here?
KUTTER: He would not have a foot.
GERTLER: Oh, yes, I`m so lucky.
SPENCER (voice-over): Despite Alfred`s happy outcome...
GERTLER: It turned out great. They did what they promised to do.
SPENCER: ... his treatment would be off-limits in Canada, or in the United States, because phage therapy never has gone through the rigorous testing the U.S. demands. Eliava`s methods hardly would pass.
(on camera): This, for example, this strikes me as fairly low-tech.
KUTATELADZE: Yes, yes, it`s very old really.
SPENCER: That`s pretty old?
KUTATELADZE: Yes.
SPENCER: You use those more than once?
KUTATELADZE: Yes, we sterilize it several times.
SPENCER (voice-over): And consider where phages are found.
KUTATELADZE: We isolate the new phage clones from sewage. Yes, it`s not a very clean place...
SPENCER (on camera): It`s not appealing either.
KUTATELADZE: ... but it has a lot of phages, so.
SPENCER: Imagine you were trying to convince an American...
KUTATELADZE: Yes.
SPENCER: ... to try a medicine that was made from sewage that had viruses in it that was used in the former Soviet Union.
KUTATELADZE: Yes, but you can trust somehow, because it works. And it has been working during so much time, so.
SPENCER (voice-over): And now, some American entrepreneurs think it`s time to give this old technology new consideration.
GLENN MORRIS, INFECTIOUS DISEASE SPECIALIST: Essentially, we`re using things that nature made, but we`re kind of adding a little high-tech.
SPENCER: Infectious disease specialist, Glenn Morris, is co-founder of Intralytix in Baltimore...
MORRIS: And so, what we do is to try to fully characterize the little fellows.
SPENCER: ... one of a few small companies starting controlled studies.
MORRIS: There is no question that on the test tube and on the culture plate, these things work like gang busters. Translating that into something that`s effective in terms of human therapy, there`s a lot to suggest that they do work. But at least in this country, we still have to prove it.
SPENCER: And that will take at least three to five years, he says, even using Eliava`s experience. And who knows where Eliava will be then?
(on camera): It`s a very impressive building.
KUTATELADZE: Yes, it is.
SPENCER (voice-over): The collapse of the Soviet Union cut off funding for research, equipment and workers. Today, Eliava struggles just to hang on to its one-of-a-kind phage inventory.
KUTATELADZE: We have some experience, and maybe other people from the world, from foreign countries, can use it.
SPENCER (on camera): When you say that, a big smile comes on your face, like...
KUTATELADZE: Yes, I hope so.
SPENCER (voice-over): There has been recent outside help...
(on camera): And this is your new equipment?
KUTATELADZE: Yes, this is our new equipment.
SPENCER (voice-over): ... including a grant from the U.S. State Department.
KUTATELADZE: So, it`s very helpful, and this is the only way to save our science and just keep going.
SPENCER: No one, not even in Georgia, thinks phages will replace antibiotics completely. But are they part of the answer when antibiotics don`t work?
KUTTER: I think we are absolutely crazy if we don`t learn to use them and to use them well and efficiently and effectively.
UNIDENTIFIED FEMALE (singing): It`s very clear, our love is here to stay...
SPENCER: One Toronto musician is convinced phages saved him, for though Alfred Gertler still needs surgery to repair broken bones, he is back on his feet and playing his heart out.
(on camera): How happy are you that you took this risk and went to Georgia and did this?
GERTLER: Well, I am thrilled. Like, I am not afraid anymore. I don`t have any despair. You know, there is medicine there. So, my prospects have suddenly improved.
(END VIDEOTAPE) (BEGIN VIDEO CLIP) UNIDENTIFIED FEMALE: Drew, fruit tonight.
ANNOUNCER: Just ahead: Children and their parents who live in fear.
UNIDENTIFIED FEMALE: A sticker. Show them what it says.
Anything related to milk, he can`t have it. Even being around eggs causes him to swell up.
ANNOUNCER: Why are potentially fatal food allergies on the rise?
UNIDENTIFIED FEMALE: "NDS" in our house is "not Drew-safe." UNIDENTIFIED MALE: Yes.
ERIN MORIARTY, CBS CORRESPONDENT (on camera): He could die?
UNIDENTIFIED FEMALE: He could. Yes, he could.
(END VIDEO CLIP) (COMMERCIAL BREAK) (BEGIN VIDEOTAPE) ADRIENNE RANDALL, DREW RANDALL`S MOTHER: Drew, fruit tonight. What do you want? I`ve got blueberries, nectarines bananas.
MORIARTY (voice-over): Whenever 3-year-old Drew Randall is invited to a party near his home in Mansfield, Ohio, his mother, Adrienne, packs him food.
DREW RANDALL, SUFFERS FROM SEVERE FOOD ALLERGIES: This!
A. RANDALL: I can`t be sure that the ones that they are going to have at the party tonight are OK, so I`ll take his.
MORIARTY: Adrienne, a special education teacher, isn`t just being picky or even overprotective. A bite of the wrong food could kill Drew.
A. RANDALL: The worst-case scenario is that he has an anaphylactic reaction that causes some kind of, like, terminal damage.
MORIARTY (on camera): He could die?
A. RANDALL: He could. Yes, he could.
MORIARTY (voice-over): Drew has severe food allergies.
A. RANDALL: He`s sensitive enough to egg that even being around eggs when they`re cooking causes him to swell up. He`s allergic to milk, and then he`s also allergic to peanuts.
JACQUI CORBA, SUFFERS FROM SEVERE FOOD ALLERGIES: I have trouble breathing, my throat feels tight.
MORIARTY: Twelve-year-old Jacqui Corba of Greenwich, Connecticut, is also allergic to peanuts. She can`t eat them or even inhale the dust from them.
J. CORBA: It feels like you`re scared that you`re going to die.
MORIARTY: And it`s not just peanuts.
J. CORBA: Sesame seeds, pumpkin seeds, sunflower seeds, poppy seeds.
MORIARTY (on camera): Eating something that was made in a factory that processes peanuts?
J. CORBA: That could -- that could kill me.
MORIARTY: Kill you?
J. CORBA: Yes.
MORIARTY: Anyone who has a child today knows someone like Jacqui and Drew. There are an estimated seven million Americans with food allergies, with an average of 200 who die every year. And while no one knows exactly why, the number of those with food allergies is on the rise.
DR. HUGH SAMPSON, ALLERGIST: There does appear to be almost an epidemic, I would say, in the last five to 10 years.
MORIARTY (voice-over): Dr. Hugh Sampson is an allergist at Mt. Sinai Hospital in New York.
(on camera): Why are we seeing so many more kids with food allergies?
SAMPSON: That`s a great question.
MORIARTY (voice-over): First and foremost, there seems to be a link between nursing mothers and eating peanuts. It may not be a coincidence, says Dr. Sampson, that 90 percent of the children who develop a serious peanut allergy, including Drew and Jacqui, were breastfed as infants.
SAMPSON: With the increase in breastfeeding, some of these children are getting exposed to very allergenic proteins. The general consensus is, we`d rather the mothers not eat peanuts while they`re breastfeeding if they`re from allergic families.
MORIARTY: This is one of Dr. Sampson`s young patients during a test for an allergy to egg.
SAMPSON: And then, you can see when we look on the rest of his body, he`s got, you know, a very itchy, red rash.
You`re really doing Russian roulette. You know, you spin the barrel each time you have a reaction, and I think that`s what generates such fear in the parents.
MORIARTY: Jacqui Corba has already had 15 allergic episodes.
J. CORBA: When we went outside...
MORIARTY: Because each one seems more severe than the last, Jacqui`s life has become ruled by food -- what she can eat and what she can`t.
DIANE CORBA, JACQUI CORBA`S MOTHER: Like, this is the nightmare right here, this section.
MORIARTY: Grocery shopping for Jacqui`s mom, Diane, has become an unpleasant, even scary ordeal.
D. CORBA: Allergy information, there it is. I`m going to look all through this.
MORIARTY: While many food manufacturers have added allergy information to their labels, and Congress is considering a law that would make it mandatory, in some cases, a silent killer is invisible.
D. CORBA: Now it says "pecans." MORIARTY (on camera): And what does it say on the allergy information?
D. CORBA: It doesn`t say anything about nuts, which is very weird.
That`s why you have to read it.
MORIARTY: Because, if you make a mistake, yes.
D. CORBA: So much for that label.
A. RANDALL: Pop tart big.
D. RANDALL: Yes.
MORIARTY (voice-over): Life is even more complicated for Adrienne Randall, whose 3-year-old son, Drew, has an even greater number of food allergies.
A. RANDALL: This cabinet is all Drew-safe. Everything in here is stuff that`s either for Drew or that Drew can eat.
MORIARTY: Because her older son, 4-year-old Jake, doesn`t have any allergies, Adrienne has had to devise a complex storage system to keep their food separated.
(on camera): What does that "NDS" mean?
A. RANDALL: This means, "not Drew-safe." This is the stuff that Jacob can pull out, like, for a snack if Drew is not around.
I have "not Drew-safe" on the top, and then, I always write it on the ingredients panel.
MORIARTY (voice-over): But keeping things safe is getting more and more difficult the older Drew gets and the more places he eats, like birthday parties.
A. RANDALL: Your sticker to remind people that they should not feed you, right? Why not? Why do they not feed you?
D. RANDALL: Because I could get sick.
MORIARTY: But even with the plainly visible sticker, Adrienne still hovers nearby.
A. RANDALL: I`m waiting to eat. Then, I won`t be so nervous.
MORIARTY: While Drew is too young to care, Jacqui knows what it`s like to be singled out for her allergy. A talented tennis player who hopes one day to play professionally, she`s best known at her middle school as: J. CORBA: "Peanut Girl." That`s me. That`s the popular one.
"Peanut Girl." MORIARTY (on camera): And how do you feel about it?
J. CORBA: I can`t stand it.
MORIARTY (voice-over): Because Jacqui`s food allergy is considered a disability, her school is required by law to keep her safe. So, at lunch, Jacqui eats in what`s called a "peanut-free zone" that includes not only her table, but the ones that surround hers.
(on camera): So you like her that much that you`ll give up that Snickers bar?
(voice-over): And even with all of the precautions, Jacqui never leaves home without her epi-pens...
(on camera): This is, like, a shot.
J. CORBA: Yes.
MORIARTY: Where does it go?
J. CORBA: It goes right in my leg.
MORIARTY (voice-over): ... disposable syringes that carry medicine, epinephrine. That could save her life in the event of a severe allergic reaction, like the one she had a year-a-half ago in a New York deli.
J. CORBA: And my mom and I asked, "So, does this have any seeds on the bun?" And they said, "No." I was about to take another bite, and I looked on the bottom, there was about four seeds.
MORIARTY: Thirty minutes later, Jacqui was in serious trouble.
D. CORBA: I saw her, and she was like gray and like the cupboard.
And she started sliding down the wall, and I just grabbed the epi-pen and just jammed it in her leg.
MORIARTY: Diane rushed Jacqui to the hospital.
D. CORBA: I think that it was the worst time of her life, but clearly, the worst time of my life. I mean, just to be in the middle of that and know that this is going to happen again.
MORIARTY (on camera): After that experience, were you hesitant to eat food at all?
J. CORBA: I was so hesitant. I -- it changed me. It changed me. I was very, very nervous to eat.
MORIARTY (voice-over): And Jacqui is still nervous.
J. CORBA: I get so nervous and full of anxiety that I create the symptoms. I still get a little shaky in New York, like eating. I don`t want to get near that street. It just scares me. I don`t want to look at that hospital.
MORIARTY: Because only 20 percent of children with peanut allergies outgrow them, Jacqui is going to have to get used to living with anxiety, which is why playing tennis has come to mean so much to Jacqui. On the court, her only risk is losing a match.
(on camera): And when you`re playing tennis, you`re not the "Peanut Girl?" J. CORBA: And I love that.
MORIARTY: You`re not worrying about your allergies?
J. CORBA: Yes, I just play my game, and it`s peaceful. It`s a great feeling to know that I don`t have to worry about that situation.
(END VIDEOTAPE) (BEGIN VIDEO CLIP) ANNOUNCER: Next: One family`s heartbreaking journey.
VAN SANT (on camera): John, just how close were you to dying?
UNIDENTIFIED MALE: As close as you can get.
UNIDENTIFIED FEMALE: I remember falling to my knees saying, `My God, what`s happening? What`s wrong?` ANNOUNCER: But it might easily have been prevented. We`ll show you how.
(END VIDEO CLIP) (COMMERCIAL BREAK) RATHER: Millions of college students have been arriving on campuses all across the country, armed with the latest tools for the information age -- laptops, cell phones, pagers and Palm Pilots -- all at the ready. But there is something else going around on campus that a lot of students and their parents may not be prepared for, although it is something a lot of medical experts say young people can and should be protected against.
Peter Van Sant now has a story of one family who got a lesson they never anticipated.
(BEGIN VIDEOTAPE) JOHN KACH, COLLEGE STUDENT: Everything was, you know, going my way.
I was happy.
VAN SANT (voice-over): In March of 2000...
J. KACH: I started concentrating on basketball, started to lift, getting my grades up, still parties, still doing my thing.
VAN SANT: ... 19-year-old John Kach was having the time of his life.
A college freshman at Salve Regina University in Newport, Rhode Island, John was on his way to becoming a star basketball player.
(on camera): What`s this picture?
J. KACH: This is when we beat Bridgewater State, I had basically the game-winning basket.
VAN SANT (voice-over): But just months after that winning basket, this 6 foot 4, 210-pound athlete lost almost everything.
John`s nightmare began when he was recovering from what he thought was the flu...
J. KACH: I was in my dorm room on a Friday night. I wasn`t feeling all that great, so I stayed in. All of a sudden, my stomach doesn`t feel right. And you know, and then I started getting real hot, fever.
VAN SANT: ... until John`s fever soared to 105, and he was rushed to the hospital.
PAIGE KACH, JOHN KACH`S MOTHER: To be that sick, to be brought to the hospital, knowing my son, John, it just gave me that funny feeling.
VAN SANT: John`s mother, Paige, was more than 150 miles away at her home in Carmel, New York, when she got a call from an emergency room doctor.
P. KACH: And he said, "Mrs. Kach, we are transporting John from Newport Hospital to Providence. He`s a very, very sick young man, and you`ve got to get here as soon as you can." I remember falling to my knees saying, `My God, what`s happening?
What`s wrong?" VAN SANT: John had contracted a rare, but often fatal form of bacterial meningitis that attacked and shut down his major organs.
DR. MITCHELL LEVY, INTENSIVE CARE SPECIALIST: There`s very little warning, and if you don`t see someone very early, it can be difficult to prevent death.
VAN SANT: Intensive care specialist, Dr. Mitchell Levy of Rhode Island Hospital, was battling the meningitis with massive amounts of antibiotics.
LEVY: His lungs were filling up with fluid, and his blood pressure was gravely low.
VAN SANT: Unable to breathe on his own, John was placed into a drug- induced coma. Within the first two days, John was given his last rites not once, but twice.
P. KACH: I remember going into John`s room, and he was under. And I remember kissing him and saying, `If you can`t do this, if you can`t make it through this, you go ahead and go. Mommy will understand. Don`t stay for mommy, because I`ll understand. But if you want to do this and you want to fight, we will fight this as a family.` VAN SANT (on camera): John was fighting a disease he most likely caught at college. Bacterial meningitis is spread through saliva, and studies show that college freshmen living in dorms are in the highest risk group.
LEVY: Why eight people can be exposed to it and only one person gets it is still a mystery to medicine. And I have seen young people come in with a sore throat and be dead within 24 hours.
VAN SANT (voice-over): And each year, more than 100 college freshmen, like John, come down with the disease.
LEVY: I thought he was going to die. I thought he was going to die, and not just when he first came in, but honestly, for quite a while after he was in the ICU.
VAN SANT: Weeks passed, and the Kach family camped out in the hospital waiting room.
(on camera): And how close are you to your brother?
MIKE KACH JR., JOHN KACH`S BROTHER: Real close.
VAN SANT: So, he`s a good friend as well as a brother?
M. KACH JR.: Best friend.
VAN SANT (voice-over): John`s 19-year-old brother, Mike Jr., remembers those painful days.
M. KACH JR.: It was like a dream. It didn`t seem like it was real.
I just waited.
VAN SANT: John`s father, Mike Sr., watched as his son wasted away.
(on camera): Give me a sense, Michael, of the shock of seeing your son, the athlete, in bed with that mask on?
MIKE KACH SR., JOHN KACH`S FATHER: Not shock as much as fear -- just pure, pure fear.
VAN SANT (voice-over): To keep their hope alive, John`s family and friends kept a journal.
P. KACH: All of your teammates have been here, and Mike has been here every day.
M. KACH JR.: "You`re my best friend and my idol. I have looked up to you since I was a little kid. I love you. Mike." VAN SANT: After six weeks of treatment, Dr. Levy decided to bring John out of the coma.
J. KACH: When I woke up, I remember Dr. Levy leaning over me, slapping his hands.
LEVY: You clapped, and you said, "John, look at me." P. KACH: It was probably one of the happiest days of my life.
M. KACH JR.: I kissed him. I said, I loved him, because that was what I was waiting to say to him the whole time. He asked me how school was going, how basketball was going. I mean, he always cared so much for me that he would always ask me how I was doing, when he was the one laying in the bed.
VAN SANT: But John`s physical ordeal was just beginning. Doctors were able to save his life, but the price was very high.
MIKE KACH SR.: I have never really begged for anything in my life, but I did beg the doctor, `Please, be as conservative and frugal as you possibly can.` VAN SANT (on camera): What are we looking at here?
J. KACH: This is my right leg. This is the one that I lost below my knee.
VAN SANT: And what are we looking at here?
J. KACH: That`s my right hand.
VAN SANT: What goes through your mind when you look at this?
J. KACH: It`s tough. You know, it`s tough to think that that`s me.
VAN SANT: That`s your right hand in this picture, and let me see your right hand now.
J. KACH: That`s my right hand today.
VAN SANT (voice-over): The meningitis prevented blood from circulating to John`s limbs, causing tissue to die. Amputation was inevitable.
P. KACH: Any parent sitting anywhere can`t even imagine how horrible it is to have somebody say, "We`re going to cut off his hands, we`re going to cut off his legs." You`re a beautiful child. You`re a gorgeous 6 foot 4, strapping, 210, handsome young man, who walks and runs and plays and jumps around and holds hands with his girlfriend. And all of a sudden, you`re going to take all of that away?
VAN SANT: What the disease couldn`t take away was John`s will.
J. KACH: It was a lot of pain. I think I could go through anything right now.
VAN SANT: He triumphed over five grueling months in rehab.
P. KACH: He said to me once, "Why me, Ma? I tried to do it all by the book. Why me?" I had no answers. I said, `Honey, I don`t know.` And he never asked me that again.
UNIDENTIFIED MALE: You can do the honors.
UNIDENTIFIED MALE: What is that?
VAN SANT: Today, with the help of his family, and these custom-made pads for his hands...
J. KACH: And my dad just made them up to fit me better. And with these, you know, I can squeeze the ball.
VAN SANT: ... John has learned to do just about everything.
P. KACH: I think he was born with something so special, and I think we were lucky enough to nurture it.
VAN SANT: As terrible as what happened to John Kach, it`s almost as agonizing to know...
J. KACH: I knew about the vaccine, didn`t get it, wish I did.
VAN SANT: ... it might easily have been prevented.
P. KACH: There is a vaccine that can prevent this kind of heartache.
VAN SANT: That`s next.
(END VIDEOTAPE) (COMMERCIAL BREAK) (BEGIN VIDEOTAPE) UNIDENTIFIED MALE: One, two, lock it. Give me one more. Come on, push, push. Come on, come on.
VAN SANT (voice-over): John Kach is working hard to rebuild his life...
UNIDENTIFIED MALE: Good.
VAN SANT: ... and his body...
UNIDENTIFIED MALE: Come on, push. Good.
VAN SANT: ... which were both nearly destroyed by bacterial meningitis.
(on camera): John, just how close were you to dying?
J. KACH: As close as you can get.
VAN SANT (voice-over): John`s close encounter with death has set him on a new mission: To let people know that most forms of the disease can be prevented with a single shot.
J. KACH: I`m here today to talk with my mom to basically get the word out about the vaccine.
VAN SANT: John and his mother, Paige, are part of a group called, Moms on Meningitis. Their message: What happened to John doesn`t have to happen to you.
J. KACH: This changed my life big-time. And you know, I don`t want to see anyone else go through what I went through and my family went through. I wouldn`t wish this on my worst enemy.
DR. JAMES TURNER, UNIVERSITY OF VIRGINIA: If you get the shot, you have reduced your risk by about 80 percent.
VAN SANT: Dr. James Turner is the executive director of student health at the University of Virginia, where all incoming freshmen are required to be vaccinated for bacterial meningitis.
TURNER: We have learned of a lot of young people`s lives who could have been saved if we had only been vaccinating years ago.
VAN SANT: The vaccine was first developed in the 1960s, after a series of meningitis outbreaks in crowded military barracks.
TURNER: About 1971, every single military recruit started receiving this vaccine, and the outbreaks of the disease virtually stopped.
VAN SANT (on camera): Today, it`s crowded college dormitories that are the breeding ground for the disease. Each year, about 100 students get sick, and a dozen die of bacterial meningitis.
Five states now mandate that all incoming freshmen be vaccinated. The cost: between $70 and $80 per student.
TURNER: It`s a god-awful disease, and I have sat in the intensive care units with the families as they have watched their children cling to life, and it`s terrible. And to think for $70 or $80, we can prevent that, it`s a no-brainer.
VAN SANT (voice-over): With virtually no side effects, Dr. Turner wants to make the shot mandatory in all 50 states.
TURNER: We have made tremendous headway in getting students vaccinated and getting information out there. Clearly, we`ve got a ways to go.
UNIDENTIFIED MALE: Nothing makes me more excited than being able to announce No. 25, John Kach.
VAN SANT: John Kach doesn`t dwell on the past. Just nine months after getting sick, John made an emotional return to visit his former teammates.
J. KACH: I just try to make my life better, people`s lives around me better, and just kind of show them, you know, there`s a lot to live for.
VAN SANT (on camera): All right, man. Show me what you`ve got.
(voice-over): Today, John is not giving up his favorite sport. He`s in training with a new goal: to make the U.S. Para-Olympic basketball team.
(on camera): Well, I`ll tell you, with all that you have been through, it`s a privilege to shoot hoops with you in this gym, man.
J. KACH: Thank you.
VAN SANT: It`s really a privilege.
(END VIDEOTAPE) (BEGIN VIDEO CLIP) ANNOUNCER: A paper cut nearly killed Bobbie Mackeon. What are her chances for a full recovery? Stay with us.
(END VIDEO CLIP) (COMMERCIAL BREAK) (BEGIN VIDEOTAPE) UNIDENTIFIED FEMALE: So, go ahead, bring your arms up above your head.
UNIDENTIFIED MALE: Breathe in. Hold your breath.
SPENCER (voice-over): Nurse Bobbie Mackeon is still struggling to overcome serious medical problems from an infected paper cut.
MACKEON: Ten years ago, we would have treated it with one drug, it would have been gone. But unfortunately, the bacteria have gotten smart.
SPENCER: In her case, oral antibiotics failed, and more drastic treatment left her with life-threatening complications.
MACKEON: I still have the pain in here that doesn`t seem to go away.
Some days are worse than others SPENCER: But today, there is good news. Her condition seems to have stabilized.
MACKEON: I can lower the amount of blood thinner I`m on.
SPENCER: And she can start working part-time.
MACKEON: I missed my patients.
SPENCER: She says, she won`t hesitate to drive home with her patients the lesson that she learned firsthand: Overuse antibiotics, and they soon may have no use at all.
MACKEON: If I can get them to understand why I don`t want to give an antibiotic for a virus, maybe my grandchildren will have antibiotics that work.
(END VIDEOTAPE) RATHER: Tonight is the last 48 HOURS I`ll be doing, at least for a while. It`s been a long, good run; more than 15 years, as one who helped create the program, and then be a reporter and anchor for it.
The original idea was to be on once a week or more in primetime, with focused, emotionally moving hours of television journalism that affects people`s lives. Not just short bursts, but full hours on one subject. And to do full hours in times of crisis -- everything from hurricanes to war.
48 HOURS has done that, and is today the third longest-running program in primetime. Some of the most accomplished, professional journalists in the world have made it so, and they`ll continue to do that.
In the season ahead, my friend and colleague, the veteran and distinguished correspondent, Lesley Stahl, will be anchoring the new 48 HOURS: 48 HOURS INVESTIGATES. Lesley and the 48 HOURS` team will take this broadcast proudly into the future.
And now, please, take a look at a preview of next Friday`s season premiere of "48 HOURS INVESTIGATES.
(BEGIN VIDEO CLIP) ANNOUNCER: A respected doctor is accused of using a patient for sex.
UNIDENTIFIED MALE: I am facing 18 years of prison for something I didn`t do.
ANNOUNCER: But this is no ordinary case.
UNIDENTIFIED FEMALE: Who is going to believe me?
ANNOUNCER: His accuser has been diagnosed with multiple personalities.
UNIDENTIFIED FEMALE: I don`t have a warning, and I -- and they just...
PETER VAN SANT, CBS CORRESPONDENT (on camera): They just appear?
UNIDENTIFIED FEMALE: Yes.
UNIDENTIFIED FEMALE: Who am I speaking to now?
UNIDENTIFIED FEMALE: (EXPLETIVE DELETED) man, you know. All right, hey, man, (EXPLETIVE DELETED) am only.
UNIDENTIFIED MALE: My life is at stake. My family`s life is at stake.
UNIDENTIFIED FEMALE: How do you do?
ANNOUNCER: You won`t believe this trial.
UNIDENTIFIED MALE: Am I talking to Vanessa?
ANNOUNCER: And, 48 HOURS did our own DNA testing with explosive results the jury never saw.
UNIDENTIFIED MALE: I never, ever had any kind of sexual contact with this lady.
UNIDENTIFIED FEMALE: Dr. Malave (ph) is lying.
ANNOUNCER: The season premiere of 48 HOURS INVESTIGATES, "A Crime of the Mind," next Friday.
(END VIDEO CLIP) RATHER: I`m Dan Rather.
As always, thank you for watching. And be sure to tune in next week for the season premiere of 48 HOURS INVESTIGATES.
Good night.
END
Content and programming Copyright MCMXCVIII CBS Worldwide Inc. ALL RIGHTS RESERVED. Transcription Copyright MCMXCVIII Federal Document Clearting House, Inc., which takes sole responsibility for the accuracy of the transcription. ALL RIGHTS RESERVED. This is not a legal transcript for purposes of litigation.
Content and programming Copyright 2002 CBS Worldwide Inc. ALL RIGHTS RESERVED. Transcription Copyright 2002 Federal Document Clearing House, Inc., which takes sole responsibility for the accuracy of the transcription.
................................